The Erosion of Medical Ethics and the COVID Holocaust
Politicized “health” has lethal consequences, from the Nazi experimentation on those considered unworthy of living, to the abandonment of the Hippocratic Oath, to today’s vaccine experimentation on entire populations.
By Lee D. Merritt MD
“The stark lesson of the Holocaust is that whenever doctors join forces with government and deviate from their personal, professional, clinical commitment to do no harm to the individual, medicine can then be perverted from a healing humanitarian profession to a murderous apparatus.” — Vera Sharav, Holocaust Survivor
America is on the brink of extermination — not because of invasion by a strong foreign army on our land (although that is possibly the end game), not because of the implementation of a Cheka-like force rounding up its own citizens (although that too is getting closer), and not because of an Apocalyptic plague ravaging the land (although that is the message the mainstream media would have you believe). No, our nation — based on individual liberty and the rule of law — is about to be conquered because “public health” and our very own public-health officials have been purposefully weaponized against us.
Two Worldviews Are Possible
There are only two worldviews that can be held regarding our current situation: Either you think public-health experts from all over the country and beyond were well-intentioned but simply wrong about everything from the wearing of masks, to lockdowns, to the benefits of hydroxychloroquine, etc., or you think what has happened to the world as a result of “COVID” was planned and orchestrated.
Deciding which of those two views is correct is aided by reviewing the controversial PCR testing program. Even non-medical, non-scientific people have become somewhat knowledgeable about the use and misuse of “PCR,” or polymerase chain reaction, tests. We have learned that these PCR tests are properly used to detect small amounts of genetic material in a laboratory setting. They were never meant for use as a diagnostic medical tool — as their Nobel Laureate inventor Kary Mullis clearly explained before his unexpected death in 2020. Nevertheless, the tests were put into general worldwide use for the diagnosis of COVID. That may be a forgivable error in a crisis — employing a “field expedient” measure not meant to last forever. On the other hand, what is not readily explainable is why the test was universally performed incorrectly.
Lab managers are highly trained professionals. They know how to read instructions. They know how to train their staff. They routinely implement new testing in their labs, and ensure that those tests are correctly performed and reported with only a few false positive or false negative outcomes. But in the entire year 2020, instead of doing what the enclosed instructions dictated, instead of cycling these tests 20-30 times, (at the most 25-35 times), every large system lab manager in the United States set the tests to cycle 40-50 times. Michael Yeadon, a former chief science advisor for Pfizer, stated that this over-cycling had the effect of producing a large number of false-positive tests — probably greater than 90 percent.
So, in one worldview, we must believe that somehow all lab managers in the United States failed simultaneously to do their jobs — and that they all erred in exactly the same way. (If by accident, why didn’t any lab manager run too few cycles to produce false negative tests?) Must we believe that some universal psychosis hit lab managers everywhere so they mistakenly produced false positive testing, and furthermore that they simultaneously awakened on Jan 21, 2021, to correct the testing procedure? Because on that day, tests were cycled below 35 times and, miraculously, there occurred a huge drop in COVID diagnoses.
There are only these two options and two worldviews: You can believe all the above, or you can believe that some authority higher up in the public health bureaucracy instructed all lab managers to over-cycle the tests. And what could have been the purpose for that instruction, except to harm the American public by grossly and falsely over-diagnosing COVID? I for one do not ascribe to the universal-lab-manager-psychosis theory.
The other worldview requires that we take a hard look at who is running our “public health.” “Public health” is a concept that only comes about when doctors become servants of the state. And nothing good has ever come of that.
Kaiser Wilhelm and the Political Use of Public Health
In the latter years of Imperial Germany, Kaiser Wilhelm’s rule was threatened by the Social Democrats. The Kaiser’s advisors at the time suggested that he give the people some boon to offset the offerings by his opponents. So, the Kaiser chose socialized, government-run healthcare. The effect at first was to get doctors and new medical procedures to underserved, impoverished areas. Interestingly, these doctors who brought with them the latest ideas from their university training were referred to as “vaccine doctors” because of the emphasis on prevention and public health.
The system worked well at first, but after WWI, as the money dried up for public programs, the medical system was left without funding but with an abundance of paperwork and cumbersome bureaucracy. Additionally, this government medical system brought about a critical philosophic change. Care that was once done on the basis of individual ethics and Christian charity was now done through a collective ethic and nationalized welfare. Government medical authorities did not deal with individual patients, but with data sets. Doctors who previously only dealt with billing individual patients became involved in the national economics of medicine, and the cost to the government of public-health issues.
This led to attempts at cost-containment through wellness. But that inevitably became cost-containment by denying treatments. The Kaiser’s medical system, like all socialized systems following it, had to ration care to some at the expense or even termination of others. In 1925, a book was authored by German lawyer Karl Binding and psychiatrist Albert Hoche: Permission for the Destruction of Life Unworthy of Life. The authors, steeped in Hegelian philosophy from the German education system, identified three groups of people unworthy to live: the terminally ill who request death, “incurable idiots,” and those in vegetative states such as trauma victims. The authors suggested a government body of doctors, lawyers, and psychiatrists who would oversee the selection of euthanasia patients by judging patients’ economic value to society and applying cost-benefit criteria. This plan separated the victims from their personal community physicians, who simply sent their medical records to a centralized, government-run committee — thus depersonalizing the decision to kill them. Community physicians, to whom these targeted people were familiar faces with personalities and real-world history, would most likely not have chosen to participate. But ultimately these doctors were not ethically absolved from consequences of the actions they set in motion. To be clear, euthanasia was not invented by the Nazis, but by physicians with legal help, then implemented by the state.
Stalin’s Use of Psychiatric Medicine
According to Lenin, government medicine was the “keystone in the arch of socialism.” In his eyes, giving people healthcare simply solidified the dependency and therefore loyalty of the masses to the Bolshevik government. By the time of Stalin, medicine had become a tool of political oppression. Dissidents in the Soviet Union, such as Zhores and Roy Medvedev, Andrei Sakharov, and Aleksandr Solzhenitsyn were too prominent to be hauled off to the gulag without a worldwide fuss, so they were declared insane and sent for “therapy” at psychiatric hospitals where they could be tortured in privacy. In 2005, Nikolai Skachkov, after protesting police brutality and corruption in Omsk, was forced to undergo a psychiatric evaluation for “paranoia.” Investigators said he was suffering from an “acute sense of justice.”
Tavistock and the Psychological Manipulation of the Masses
“The conscious and intelligent manipulation of the organization, habits and opinions of the masses is an important element in democratic society. Those who manipulate this unseen mechanism of society constitute an invisible government, which is the true ruling power of our country.” — Edward Bernays, from Organizing Chaos
In 1921, the 11th Duke of Bedford, Marquess of Tavistock, gave a building to what was to become the Tavistock Institute. The purpose was to examine the effect of “shellshock” on British WWI veterans and to examine the limits of human psychological endurance. Later, the Tavistock Institute in London officially became a think tank that used Freudian principles to sway the public toward certain social — some would say socialist — ideas. What began as manipulation of individual behavior was expanded to group manipulation, and then generalized to populations. Tavistock’s Brigadier General Dr. John Rawlings Rees applied this concept to warfare, including civilian populations, describing “A controlled Psychological Environment.” Now, in the 21st century, the military lingo is “perception management,” and is part of “unrestricted warfare.”
Mind control for people control: Edward Bernays, an early 20th-century pioneer in the field of propaganda and mass manipulation, is known for his work in promoting Lucky Strike cigarettes to women. Bernays-style mind control has affected the medical community as well.

In 1999, Chinese PLA Colonels Qiao Liang and Wang Xiangsui outlined the concepts of unrestricted warfare in the book Warfare Beyond Rules: Judgement of War and Methods of War in the Era of Globalization (translated as Unrestricted Warfare). Psychological manipulation of populations is frankly discussed as a component of multidimensional stealth war involving, for example, cyberattacks, economic attacks, bio and chemical weapons, and political manipulation. Recently, in America, the Journal of Information Warfare included an article entitled “The Flexibility of Official Information during Contemporary Conflicts,” by information-security expert William Hutchinson. The abstract suggests that governments and militaries of Western nations have practiced “perception management” on populations worldwide for decades. Ironically, but not surprisingly, when you click the “Read the Article” button to get more details, you are told “Access Denied. You are not authorized to access this page.”
According to Dr. John Coleman, in an excellent monograph written in 2005 entitled The Tavistock Institute of Human Relations: Shaping the Moral, Spiritual, Cultural, Political and Economic Decline of the United States of America,
Tavistock member Edward Bernays, a nephew of Sigmund Freud, is considered the father of modern publicity. One of his more famous campaigns was a 1929 promotion of female smoking by branding cigarettes “Torches of Freedom” — equating them with feminism and emancipation of women. But Bernays is less well known for his more insidious propaganda and mass mind control. In 1955, Bernays wrote a book about his experience entitled The Engineering of Consent. From Dr. Coleman’s monograph:
As a major player in the Deep State, the Tavistock Institute has extensive personnel ties to U.S. research and advisory entities such as MIT, the Stanford Research Institute, the Heritage Foundation, Georgetown University’s Center of Strategic and International Studies, and the Rand Corporation. According to an October 26, 1963 article in Business Week, psychological testing programs and group relations training programs of the institute were implemented in the United States by the University of Michigan and the University of California. “Group relations training” may sound harmless or even beneficial, but beyond political manipulation, or getting people to buy a certain product, 21st-century “perception management” is nothing short of group “mind control.” This “mind control” can be practiced upon the entire population or upon groups of physicians and public-health “experts.” In short, a few people in the world can bring about their desired outcomes by orchestrating behavior of the masses, including doctors and researchers.
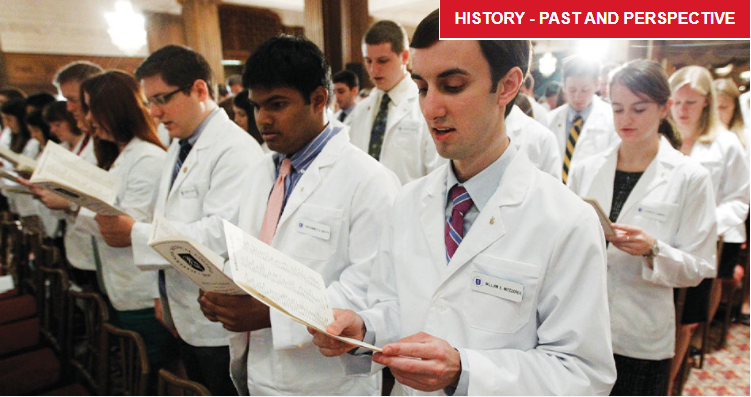
What About the Hippocratic Oath?
To understand the ethical decline of the practice of medicine, we need to look first at the structure of medical practice that facilitated the changes. Up until the last three decades, over 60 percent of physicians were in some form of private practice. In the 1990s, under the pressure of 160,000 pages of Medicare regulations, doctors began selling their practices to large corporate medical conglomerates. With the adoption of the new healthcare distribution system commonly known as “ObamaCare,” the exodus from private practice became a stampede. Today, most physicians are working under the aegis of a hospital or large healthcare system. Roughly 70 percent of the funding for those hospitals and health systems comes from government. And what the government funds, the government regulates.
Treatment of the sick during the year of COVID was not planned and executed by doctors at the patient’s bedside, but by medical authorities at a distance, sending their “guidance” to medical administrators. Physicians who disagreed with the pronouncements of the U.S. Centers for Disease Control and Prevention (CDC) were marginalized, cancelled from their contracts, or fired. Hospital administrators and their myriad underlings — none of whom take a sacred oath to protect patients — enforced National Institutes of Health (NIH) and CDC demands. In my area, hospitals would discharge patients (sometimes threatening to do so in the middle of the night) who did not want to take the authorities’ recommended remdesivir — a drug that had no track record of success against COVID. In nearly all hospitals, standard care such as breathing treatments for lung problems was not instituted, citing concerns of spreading COVID. On the other hand, private physicians who had “done their due diligence” and read the basic science, and had studied the success around the world with hydroxychloroquine and ivermectin, tried to do the right thing. However, they were usually overruled by pharmacists who refused to fill the prescriptions. I had a pharmacist tell me she “morally disagreed” with the hydroxychloroquine prescription and refused fill it.
Some of this can be attributed to overt bribery. The more than $400 billion that crossed Dr. Fauci’s desk over the last 40 years, along with other NIH grants, allowed teaching hospitals and research institutions to expand beyond their normal means. Now, refusing to implement CDC guidelines or Fauci’s edicts could lead to losing next year’s money flow.
But this does not explain the stubbornness with which individual physicians fought against any treatment of COVID and instead pushed experimental vaccination. This doesn’t explain the many nursing-home deaths attributable to medical neglect. After Indonesians and others showed the profound effect vitamin D levels had on the survivability of COVID, why were doctors not giving that cheap supplement to nursing-home patients? A simple prophylaxis of vitamin D, vitamin C, NAC, zinc, and two hydroxychloroquine tablets a week — as was done in third-world countries that dispensed “home COVID kits” — had the potential to reduce mortality by 250,000 people in the United States, based on studies pooled for the online HCQtrial.com.
There is killing by “commission” — doing something to kill a person — and there is killing by “omission” — purposefully withholding treatment that could save life. In either case, the physician is failing his traditional ethical duty. As Die-trich Bonhoeffer opined, “Silence in the face of evil is itself evil: God will not hold us guiltless. Not to speak is to speak. Not to act is to act.” How did American medicine get to this place?
Medical ethics has been under assault, and not by accident. It has been subtly degraded along with the purposeful warping of the public consciousness as discussed above.
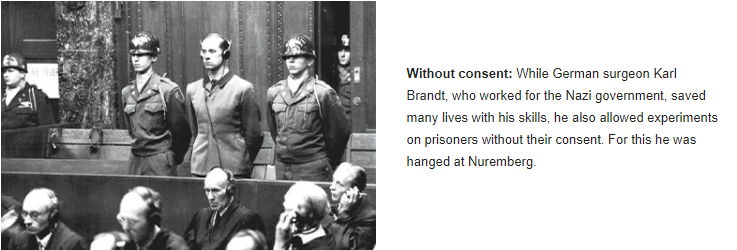
Without consent: While German surgeon Karl Brandt, who worked for the Nazi government, saved many lives with his skills, he also allowed experiments on prisoners without their consent. For this he was hanged at Nuremberg.
The Oath of Hippocrates has been the bedrock of Western medical ethics for millennia, but in the last half century, the oath has been slowly eroded until it no longer exists, except in theory. The Hippocratic Oath I took in 1980 has been “modernized” mostly to leave out those uncomfortable prohibitions against abortion and “cutting for stone.” The latter amendment is a practical matter that no longer pertains to the age of specialization and aseptic surgery, so that revision can be justified as a technical clause. But the former speaks to the ethical role of physicians in the preservation of life. And, lest we forget, professional ethics is the sole point of the Hippocratic Oath. In the last 20 years, the oath has been doctored (pun intended) and distorted to the point of unrecognizability. As Dr. Jane Orient, executive director of the Association of American Physicians and Surgeons, reported in her 2011 article “Roll Over Hippocrates,” the first graduating class of the Phoenix branch of the University of Arizona College of Medicine was assigned the task of writing their own oath.
The key to Hippocratic ethics is the independence of the physician. He is not a servant of the state, but of his patient. “Into whatever houses I enter I will go into them for the benefit of the sick and will abstain from every voluntary act of mischief and corruption.” “For the benefit of the sick” does not mean for the bottom line of government or the pharmaceutical industry. And when it states, “I will follow that method of treatment which, according to my ability and judgment, I consider for the benefit of my patients,” it does not put the CDC guidelines or the hospital’s rules above the welfare of the patient. Generations of doctors have now been led to believe many pernicious things:
- Science is by consensus, independent thinkers need not apply;
- Following authorities’ guidelines results in the best outcomes;
- Accepting information put forth in approved medical journals is the way to avoid “quackery”;
- “Evidence-based medicine” comes from statistically significant double-blinded trials — evidence cannot be adequately found at the bedside by direct observation;
- Experience is always inferior to published data; and
- The most devastating notion that has been adopted in the last several decades: public health trumps the care of the individual.
The often-overlooked point in the oath, but one critical to understanding the ongoing medical nightmare of COVID, is the constant reference to “the patient.” The oath — and the doctor’s moral obligation — is not to a group, nor to the common good, nor to the state. It is to the individual patient of the individual doctor.
I have written and spoken extensively about Karl Brandt, who was Hitler’s surgeon and head of the Reich Medical Department. (See “The Lessons of Karl Brandt,” https://www.jpands.org/vol16no1/hieb.pdf). Dr. Brandt personally saved many lives by performing surgery and improving the trauma system during the war. But, as the officer nominally in charge over doctors who experimented on prisoners in the death camps, he was hanged after the Nuremberg Doctors’ Trial for “Conspiracy to commit Crimes Against Humanity.” His crime was allowing prisoners to be experimented upon under coercion and without informed consent. Informed consent requires honest disclosure of the risks, and the ability to opt out without penalty. These experiments, and other acts that would be considered immoral or professionally unethical when done individually, were justified “for the good of the state.” Brandt was educated to believe that the collective took precedence over the rights of the individual — a sentiment he took with him to the gallows. And this is the ethical worldview being adopted by our medical system today.
The concept of public health is not in itself evil, but sacrificing a few individuals for the greater good, in the name of public health, is ultimately evil.
How We Take Back Our Medical Ethics
Doctors are at a crossroads. As professionals, we can do as our German predecessors and ride the bus over the moral cliff. Or we can get off. In 1943, with bombs dropping on their heads and people needing emergency treatment, it may have been harder to take that leap off the bus. But today, the choices are clear.
All physicians must stop pushing unproven, unauthorized genetic therapies (i.e., mRNA “vaccines”) upon an unsuspecting public, using coercion and without informed consent. Physicians, whether or not they believe the vaccine to be good or bad, cannot deny the fact that patients are being coerced (reduced prison sentences, ability to keep a job, ability to travel, ability to attend college etc.), and that they are not given true informed consent (in most cases they are given no informed consent whatsoever).
Doctors must educate themselves, not blindly accept the word of some medical authority about treatment and preventive strategies available. By the Oath of Hippocrates: “I will follow that method of treatment which, according to my ability and judgment, I consider for the benefit of my patients, and abstain from whatever is deleterious and mischievous.” This part of the oath is a commandment to study. Judgment requires education. There are now hundreds of peer-reviewed, and many more not “peer reviewed,” scientific papers that demonstrate the significant life-saving benefit of early treatment with re-purposed drugs such as ivermectin and hydroxychloroquine — drugs that have been widely used for years and for which safety profiles are well known. To continue to follow guidelines while failing to study for oneself is to violate the moral duty of a physician.
Physicians must stand together publicly on the side of ethical medicine. When the Germans invaded Holland in WWII, they demanded the Dutch doctors take part in the German medical system, including euthanasia. The Dutch doctors, who were private practitioners and who knew their patients as community members, family, and friends, were horrified and refused. When the Germans threatened to take away their licenses, all the Dutch doctors freely relinquished their licenses rather than participate in the immoral German medical system.
Big Medical: Private physicians’ practices have been largely replaced in the United States by large hospital networks. Most doctors are now beholden to “the system” rather than their patients. (Photo credit: EyeMark/iStock/GettyImagesPlus)

Ultimately, when medical care is given to you by the state, the state controls what care you receive. And therein lies the ultimate truth of COVID — we are being controlled by the technocrats of Public Health. COVID and the “vaccine holocaust” did not start in 2019. This is the result of 150 years of progressive manipulation of public opinion to condition doctors and the general public to accept policies ultimately detrimental to the well-being of humans and the future of humanity.
As long as doctors work for a hospital, the government, or a big conglomerate, they do not work for their patients. Free medicine is not free. It is theft from some people for the benefit of others. All the government does is determine who is robbed and who is benefited. And in the process, medical care becomes so overregulated and micromanaged that it becomes expensive and is less available for everyone except the elite. Worse than that, governments routinely participate in mass murder, and they have used physicians and the guise of “public health” to do it. Physicians should look at their situation. Did their institution kill people by neglect or mistreatment or coerced vaccination? And no matter the financial consequences, are they willing to continue to participate?
It is time to reclaim our profession. It is time to get off the bus.
Dr. Lee Merritt has been in the private practice of orthopedic and spinal surgery since 1995, has served on the board of the Arizona Medical Association, and is past president of the Association of American Physicians and Surgeons.
Published with Permission of thenewamerican.com