Washington bureaucrats dictate genocidal hospital protocols that exaggerate Covid mortality, boost official narratives, and leave families devastated.
Covid Hospitals: The New Killing Fields?
By Rebecca Terrell
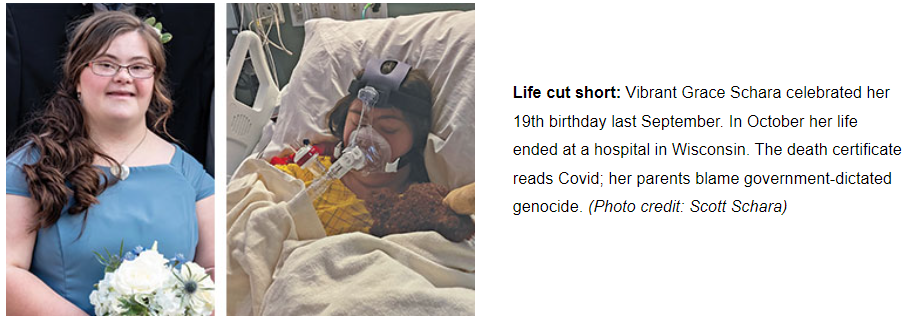
Imagine that doctors tie your daughter down to a bed and administer increasing doses of drugs in a lethal combination until she turns cold, stops breathing, and dies. That horrifying scenario is what the father of 19-year-old Grace Schara described as happening — not in 1940s Nazi Germany — but last October in a Wisconsin hospital.
The U.S. Centers for Disease Control and Prevention (CDC) now numbers Grace among more than one million Covid deaths nationwide in the past two years. Seven days before she died, the hospital admitted her with Covid, but her father believes the drug overdose, not the disease, killed her. Many medical professionals he has consulted agree.
“I’ve come to the conclusion that they may have taken her life because she had Down syndrome,” Scott Schara told The New American. As Grace’s patient advocate under the Americans with Disabilities Act (ADA), he was able to stay with her in the hospital — a rare occurrence in today’s Covid wards. There he witnessed what he thinks was a rigorous and organized agenda to end her life.
This is Scott’s painful story: Even until early the day she died, Grace was able to communicate and care for herself. Her store-bought pulse oximeter showed blood oxygen levels safely above 90 percent despite repeatedly low readings from hospital monitors — sometimes more than 40 points off — and staff conceded the errors. A doctor also wanted to intubate Grace because of lab results that Scott questioned; upon review, the physician agreed it was unnecessary, leaving her instead on a non-invasive oxygen mask, called a BiPAP. Regardless, the hospital pushed four more times for family pre-approval for a ventilator, in case she needed one and staff couldn’t reach the Scharas. The family emphatically refused because Grace’s doctor admitted drastically low survival rates of intubated patients. However, Scott documented nurses preventing him from helping Grace eat because of the BiPAP mask; doctors later cited her malnourished state as reason to convince the family she needed a feeding tube.
Three days prior to Grace’s death, an armed guard escorted Scott from the hospital. An administrator told him it was because he had been turning off Grace’s monitor alarms. He admits having done so, but only with nurses’ permission and per their instructions so Grace could sleep at night. When he objected to leaving, the administrator claimed that the nurses wanted him to leave, though how they could trump the ADA — let alone Grace’s needs and wishes — was not discussed. Scott recalls how sad she was as he kissed her goodbye; neither of them knew it was the last time they would see each other. Later, the hospital sent Scott a letter claiming he was removed because he had tested positive for Covid, but staff had warned him that he would likely get Covid in the hospital, and he had indeed tested positive three days before they removed him.
He had to enlist the help of a special-needs attorney so Grace’s older sister, Jessica, could act as patient advocate in his stead. (His wife, Cindy, had Covid at the time, too, so could not take his place.) “The total gap without coverage was about 44 hours,” Scott calculates. But Jessica’s arrival cheered Grace, and the sisters spent time together, visiting and FaceTiming with family. In phone updates to Scott and Cindy, the doctor even commented on how well Grace was doing.
Nevertheless, hospital staff twice told Jessica she had to leave Grace’s room — on her first evening, due to a miscommunication about Jessica’s patient-advocate status, and early on the day of Grace’s death, when Jessica wanted to take a shower (though they never made Scott leave for that reason). Upon her return, Jessica overheard doctors talking in the hallway.
“The family isn’t going to like this,” she recalls them saying. When asked, they told her they had to strap Grace to the bed because she wanted to use the bathroom.
Jessica entered to find her sister sedated. Throughout the morning doctors had been upping doses of a tranquilizer they had been giving Grace for four days without the family’s knowledge. Precedex is normally used as anesthesia for surgery or ICU sedation, and its package insert warns against administering it for more than 24 hours. On the day of her death, between midnight and 10:48 a.m., Grace received 14 times her initial dose, according to Scott’s calculations from hospital records he obtained later. At 11:25, nurses gave her a dose of the benzodiazepine sedative lorazepam, followed by two additional doses within three minutes of each other, at 5:46 and 5:49 p.m. Less than 30 minutes later, a nurse administered a rapid injection of morphine, a narcotic that comes with a package insert warning of the high risk of death if it is combined with benzodiazepines or sedatives. The insert also instructs caregivers to have the antidote medication naloxone “immediately available” in case resuscitation is needed. Scott says Grace’s doctors ignored this precaution.
At 7:20 p.m., Jessica called her parents in a panic over Grace’s plummeting vital signs. Scott and Cindy urged her to get help, but she told them that the nurses refused to enter the room. One of them informed her that Grace had a DNR [do not resuscitate] order that prevented them from intervening.
“She’s not DNR! Save our daughter!” Scott and Cindy yelled from the FaceTime call on Grace’s phone. But no nurse stepped up. “Are you not helping our little girl because she has Down syndrome?” Cindy shouted.
Within minutes, it was too late. “We watched Grace die on FaceTime at 7:27,” Scott recounts. Devastated, Jessica lay down next to her sister in bed, and for the next 20 minutes, she says, an armed guard who had been stationed outside the room during the entire ordeal stood watching her. Later that evening when Cindy went to the hospital to collect Grace’s belongings, one of the nurses whispered to her, “Me and several of the other nurses don’t think Grace should have died today.”
The hospital has not responded to several interview requests from The New American.
20/20
Hindsight is torture for the Scharas, adding crushing pain to their loss. Scott says if he had known then what he knows now, his daughter would still be alive. He cannot explain why a hospital would dictate care based on faulty medical equipment, isolate Grace from ADA advocates, prevent her from eating to the point that she needed a feeding tube, restrain her, unilaterally label her DNR, administer an ICU sedative for an extended time, and finally combine it with narcotics that rapidly ended her life.
Scott believes that the hospital sedated Grace in order to classify her as ICU, making it difficult for the Scharas to take her home had they tried. He thinks doctors then used the feeding tube as an excuse to increase the sedative. He also declares Grace’s DNR status counterfeit. As her powers of attorney, her parents had not signed a DNR agreement; even if they had, their phone appeal was enough to revoke it, Scott discovered later when reviewing state law.
But the issue of restraints got him thinking. Did staff strap Grace down for her safety or for their own convenience? Scott later discovered that laws governing the use of restraints are extremely strict. “Do you think that you would have been strapped down if you were in the hospital?” he recalls his attorney asking. “No, I wouldn’t have,” he answered, and told The New American that was when he realized doctors took advantage of Grace’s inability to stand up for herself.
Scott obtained her medical records and counted 36 references to Down syndrome in 22 doctors’ reports. Three times doctors asserted that they could not converse with her, though according to Scott “Grace communicated well until sedated her last day.” He read two negative allusions to her weight — 180 pounds — claiming that it would hinder staff from caring for her properly.
The hospital refused to meet with Scott and Cindy regarding their concerns, so the couple decided to go public, posting their story at OurAmazingGrace.net. Still not certain of the facility’s motive, Scott maintains that “rationed care … is an elitist proposition” that “fits like a glove” with the global population-control agenda, of which his daughter was a victim. “If the government wants to take out the disabled and the elderly,” he noted, “they can use the hospital system without admitting this.” He pointed out that as soon as patients check in, hospitals “instantly know if they’re on Medicare (elderly) or Medicaid (disabled).” Grace’s Down syndrome put her in the latter camp.
“I agree the medications killed your daughter,” an intensivist told Scott after reviewing Grace’s records. “What happened to Grace is awful and scandalous; unfortunately, this is what is happening across the country. Hospitals have become dangerous places for patients.”
In the Trenches
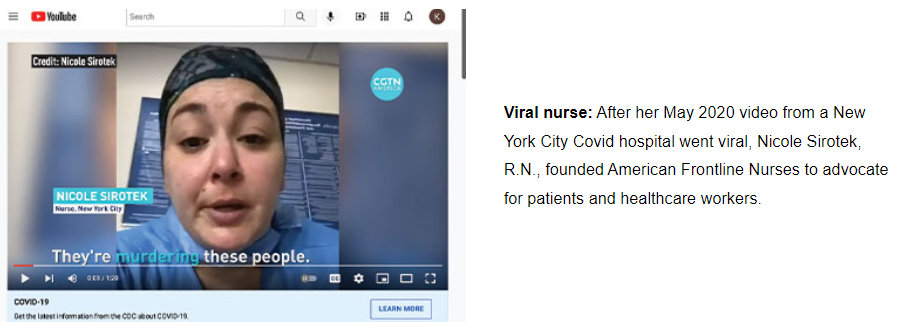
“I didn’t see a single patient die of Covid,” said Nicole Sirotek, founder of American Frontline Nurses (AFN), during testimony on Capitol Hill in January. “I’ve seen a substantial number of patients die of negligence and medical malfeasance.”
It bears repeating that she “didn’t see a single patient die of Covid,” because Sirotek, a registered nurse and biochemist, served on the frontlines of New York during the height of the pandemic and elsewhere since. As she made the claim, fellow healthcare workers sitting nearby nodded in agreement. They were all part of a panel discussion, “COVID-19: A Second Opinion,” hosted by U.S. Senator Ron Johnson (R-Wis.).
Sirotek accused hospital administrators of teaming with federal health officials and pharmaceutical companies to isolate and victimize Covid patients. She contrasted the situation with her experience working in “hot zones” in South America, India, and South Africa, where she helped stop viral spread with early interventions that U.S. bureaucrats prevent Americans from receiving. “Nowhere in those countries … do I see these issues that we see here in the United States,” Sirotek asserted. “I tell people you are better off in South America in a field hospital than you are in Level 1 trauma designer hospitals in the United States.”
In stunning parallel to Grace’s case, Sirotek complained of hospitals regularly using the BiPAP mask as an excuse to starve patients. “Well that’s what us nurses are for. We’re going to help you take your BiPAP mask off, and we’re going to help you eat. But we’re not allowed to,” she charged. “Why do I need to get a court order to force a hospital to feed a person who isn’t intubated and who is literally telling you they would like food?”
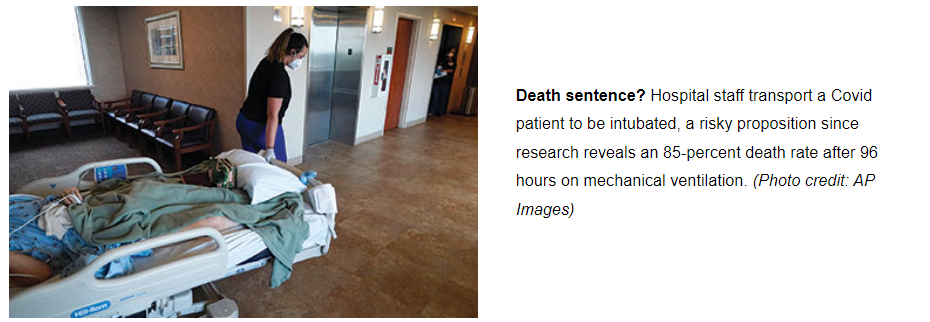
Once on a ventilator, victims fare worse. “I’ve had patients that haven’t been bathed, haven’t been fed, haven’t been given water, and haven’t been turned. And if you ask me, this isn’t a hospital, this is a concentration camp,” Sirotek stated. “Nowhere in the United States do we isolate people for hundreds of hours at a time with no human contact. It’s not even allowed in the prisons.”
“Prisoners in American jails have more visitation rights than do COVID patients in American hospitals,” wrote Dr. Lee Vliet in an October op-ed for WorldNetDaily. A medical doctor and author, Vliet recounted numerous other human-rights violations that would not pass muster of the post-World War II Geneva Conventions to prevent abuse of prisoners. Her descriptions read like a duplicate recount of the Scharas’ experience. She reported that hospitals routinely deny Covid patients adequate fluids and nutrition. They “suffer inhumane isolation with use of chemical and physical restraints,” while facilities employ law enforcement “to deny access to hospital grounds for family and advocates.” She also cited autopsies confirming that many patients died from lack of standard medicines such as blood thinners and steroids.
Equally damning is the fact that hospitals are pushing ventilators and toxic drug treatments, not with patient health in mind, but with the promise of big payoffs for following federal Covid protocols. In an op-ed posted at the nonprofit Truth for Health Foundation website, Vliet and attorney Ali Shultz dub the government incentive payments “Biden’s Bounty on Your Life.” Examples of these handouts include the “New COVID-19 Treatments Add-On Payment” system of the Centers for Medicare & Medicaid Services (CMS). This hospital incentive program is effective “until the end of the COVID-19 public health emergency,” which President Biden extended indefinitely in January, despite the nearly universal rollback of Covid restrictions across the country and around the world. The 2020 Coronavirus Aid, Relief and Economic Security (CARES) Act also provides financial bonuses to hospitals on the condition that their Covid-related treatments follow the strict dictates of the National Institutes of Health (NIH).
What are some of the incentives bureaucrats use to lure avaricious hospital executives down the genocidal path? Vliet and Shultz list a few:
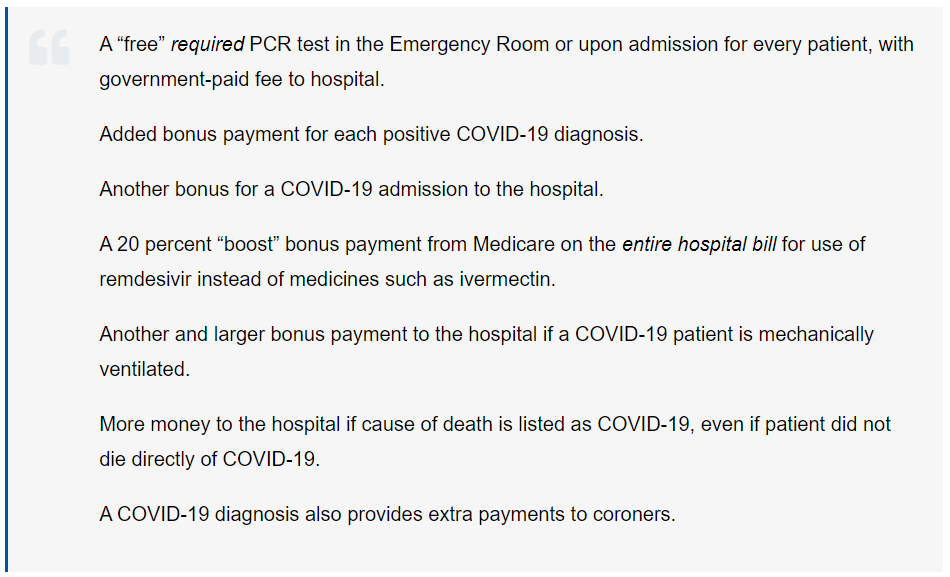
Remdesivir, the Medicare bonus drug mentioned above, has become a familiar and infamous term since April 2020 when Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases (NIAID), gave a thumbs up to the antiviral drug six months prior to completion of his agency’s clinical study, the Adaptive COVID-19 Treatment Trial (ACTT). He justified the jumpstart, claiming preliminary results were quite promising, though they were not peer reviewed, nor did he bother to publish them. The next day, the U.S. Food and Drug Administration (FDA) granted emergency use authorization (EUA) to the experimental medication for hospitalized Covid patients
Fauci kept mum about results of another NIAID-funded study, the PALM Clinical Trial, published only five months prior in the New England Journal of Medicine, just before SARS-CoV-2 emerged. Investigators had studied four drugs, including remdesivir, for treatment of Ebola virus. They terminated remdesivir early, finding it “much less effective at preventing death,” according to an NIH press release. That was a disingenuous way of admitting that more than 50 percent of the trial’s remdesivir patients died early in the investigation. An analysis of the data also shows the drug caused extensive kidney damage.
Another study on the toxic medication involved Covid patients in China and, ironically, was published in The Lancet on the same day in April that Fauci boasted of remdesivir as the new “standard of care” in the United States. Researchers reported that they had to halt investigations early — they claimed difficulty in recruiting patients despite a worldwide pandemic — but their partial findings concluded that “remdesivir was not associated with statistically significant clinical benefits.”
Nevertheless, at the conclusion of the ACTT trial in October 2020, FDA reaffirmed its authorization, even extending EUA to children. Didn’t that fly in the face of clinical results?
“What Dr. Fauci did not tell you was that the primary end-point of the study was changed half-way” through the trial, explained Dr. Paul Marik, pulmonary specialist and chairman of the Front Line COVID-19 Critical Care Alliance (FLCCC) in Capitol Hill testimony in January. Charging them with scientific misconduct, Marik said researchers invented a “bogus endpoint” to generate positive results, despite multiple independent studies that have since validated the PALM findings of increased risk of death and kidney failure. Even the World Health Organization (WHO) published a November 2020 recommendation “against the use of remdesivir … regardless of disease severity.” Marik warned, “The federal government is incentivizing hospitals to prescribe a medication which is toxic.”
“We all saw it was killing the patients,” Sirotek recalls of what she and other nurses witnessed on the front lines in New York. She said AFN research reveals that patients’ chances of survival decrease significantly after two doses. Yet, in January 2022, the FDA extended EUA of remdesivir to non-hospitalized individuals — even infants — who test positive for Covid. “We are going to see the amplification of death across our country,” Sirotek predicted.
Meanwhile, remdesivir manufacturer Gilead Sciences, Inc., is cashing in on its government-sanctioned monopoly. Days after FDA’s first approval, NPR announced that Gilead was “donating its initial supply of 1.5 million doses,” but would have to start charging once that was exhausted “to make production sustainable.” That’s a laugh, considering that American taxpayers footed most of the R&D bill. According to a March 2020 briefing note from Knowledge Ecology International, the U.S. Army, CDC, and NIH/NIAID “either conducted or funded much of the preclinical and clinical development of remdesivir,” which it quoted Gilead Chairman and CEO Daniel O’Day loosely estimating as costing “billions of dollars” over the previous decade.
Fast-forward to February 2022, when RealClearMarkets reported that remdesivir “claimed the top spot for hospital drug spending in 2021, with sales earning Gilead $4.2 billion in the first nine months alone.” For a drug that kills patients, that’s a double hit to American taxpayers. But it’s a double return to Gilead investors interested in progressivist policies, such as the population-control-promoting Bill & Melinda Gates Foundation and BlackRock, the asset-management behemoth with a stated goal of global “decarbonization.” (That’s insider code for depopulation, as Llewellyn King, host of PBS’s White House Chronicle, practically bragged in a December op-ed published at InsideSources.com.)
Sheep’s Clothing
The windfall comes as no surprise to those who have perused the federal government’s Covid-19 Treatment Guidelines, available on the NIH website. They were composed by a panel of medical experts, 40 percent of whom receive funding from, hold stock in, and/or serve as consultants/advisors to pharmaceutical companies. The “Panel Financial Disclosure” lists seven members with ties to Gilead through research support and consultancies. One panelist even serves on Gilead’s advisory board.
Vliet says their recommendations fall in lockstep with the “Complete Lives System” of President Obama’s senior White House Health Policy Advisor Dr. Ezekiel Emanuel, brother of Obama Chief of Staff Rahm “Never-Let-a-Crisis-Go-to-Waste” Emanuel, and one of the main architects of ObamaCare. He published his rationed-healthcare proposal in The Lancet in 2009, admitting that it prioritizes “younger people who have not yet lived a complete life” while reducing “chances for persons who have lived many years.”
His vision became reality in 2010 when the Affordable Care Act established an Independent Payment Advisory Board (IPAB), a panel of medical experts with unchecked control over decisions to provide or withhold treatments in order to control Medicare and Medicaid spending. Then-U.S. Representative Michele Bachmann (R-Minn.) recognized Emanuel’s fingerprint and accused him of planning healthcare rationing by age and disability, prompting former Alaska Governor Sarah Palin to wonder if his “death panel” would deem her Down syndrome son “worthy of medical care.” Had Congress not repealed IPAB in 2018, its mandates would be exempt from judicial overview and could only be overturned by majority votes in both the House and Senate and the president’s signature.
That sounds alarmingly like the current Covid-19 Treatment Guidelines panel, which, unfortunately, gets less press. Vliet also compared Emanuel’s Complete Lives System — and current Covid protocols — to England’s infamous Liverpool Care Pathway (LCP), in place from the late 1990s until 2014. Peddled as a death-with-dignity protocol, it turned out to be a method of murder through over-prescription of painkillers or starvation and dehydration. BBC News reported in 2013 on 90-year-old Kathleen Vine, who went to the hospital with a dislocated shoulder. Within a short time, the hospital called her family to tell them she had 48 hours to live. Vine’s adult granddaughters intervened to find her begging for food and water. Predictably, she recovered under their care. “I was being left to die,” Vine told BBC. “If it hadn’t been for my family, I would be dead now. I would just have been another statistic on the books.”
Fortunately for Vine, her family could visit her in the hospital. That luxury is not available to most hospitalized Covid patients. However, in striking analogy to Covid facilities, U.K. hospitals received millions in National Health Service incentive payments for reaching LCP quotas of patients “allowed” to die, as revealed by a 2012 Freedom of Information Act request by The Telegraph. Many of the recipient facilities reported that expected deaths skyrocketed under LCP, some more than doubling over previous years.
U.K. journalist Jacqui Deevoy asserts that LCP is now back in full force since the advent of Covid. “I realized something was wrong when I found out last year that my dad had a DNR put in place,” she relates in her 2021 documentary A Good Death? Her father, age 76, didn’t know about his DNR either. Her further investigation revealed that hospitals were practicing an updated version of LCP, using a lethal cocktail of drugs coupled with starvation and dehydration. Her video features stories of the Covid-era euthanasia protocol’s victims and their loved ones, whistleblowing healthcare workers, and incriminating government documentation.
Across the pond, Biden named Dr. “Death Panel” Emanuel to his transitional Covid-19 Advisory Board in 2020, prompting The Wall Street Journal to recall his Obama-era plans and a 2014 op-ed he penned for The Atlantic. In it he claimed that people who live “too long” become “feeble, ineffectual, even pathetic.” He pegged 75 as the ideal age to die.
“Can we expect that opinion to influence his pandemic-board work where life and death decisions will be made?” wondered the Journal. No need to speculate about that. In March 2020, just two weeks after WHO declared a global pandemic, Emanuel and a team of his cronies published “Fair Allocation of Scarce Medical Resources in the Time of Covid-19” in the New England Journal of Medicine. Reading like a “Complete Lives” revisited, the article recommended prioritizing medical care for those with “instrumental value” and “reasonable life expectancy.” Elderly and disabled need not apply.
More recently, Emanuel garnered 300 signatures on an open letter he broadcast on his blog in January, praising Anthony Fauci for “guiding the country to very successful outcomes” over the past two years and condemning Fauci’s critics as partisan distractors. In response, the Association of American Physicians and Surgeons (AAPS) conducted an informal survey to gauge public reaction. “Within two days, 900 doctors had responded, of whom 90 percent said they ‘strongly disagreed’ with the letter.” Ninety-six percent of the more than 6,000 non-physician respondents also strongly disagreed. Many commenters noted that the letter expressed exactly “the opposite of what front-line workers are seeing.” One physician asked “how much money the signatories are collecting in research dollars” under Fauci’s purview.
Do No Harm
There is no need to speculate about the Covid bonanza for hospitals. The website ProtocolKills.com provides a per-state list of taxpayer dollars hospitals receive for each Covid case, based on documentation from sources such as Becker’s Hospital Review and the Greater New York Hospital Association. West Virginia earns top billing at $471,000, while New York garners a relatively paltry $12,000. The average is $171,000 per case, with fluctuations based on whether the patient receives remdesivir, is put on a ventilator, and other variables.
Was that why the hospital where Grace Schara died was pushing so hard for permission to intubate her? Once the family refused, her father concludes, “It’s probable that Grace was worth more to the hospital dead than alive.” Her Medicaid invoice showed the facility was paid only $1,680 per day since she was not on a ventilator, while the bonus for her death was $13,000. Had she been cured, they would have received nothing. Schara estimates that the health system to which that hospital belongs raked in more than $8.4 billion in CARES Act bonuses and Covid death payments in one year alone, all courtesy of the American taxpayer.
Since hospitals have obviously become mercenaries for the genocidal government agenda, are we left without healthcare options? Certainly not, thanks to groups such as FLCCC (covid19criticalcare.com), AAPS (aapsonline.org), and America’s Frontline Doctors (americasfrontlinedoctors.org), which offer home-based Covid treatments and even telemedicine services for those who lack access to a sympathetic local physician. The website c19protocols.com conveniently lists most of those options. Not only can they save lives, they can also serve as an inspirational wake-up call to those of us who are acclimated to a nanny-state that dictates deadly regulations. Our personal healthcare decisions are no business of any government bureaucrat. Cutting the apron strings will prove the healthiest cure for Covid ills.
Rebecca Terrell is a senior editor of The New American.
Related articles:
Her Light Shines On
Crazy ‘Bout Elvis
Published with Permission of thenewamerican.com