How COVID Vaccine Spike Proteins Damage Your Body
Spike Protein Damages Vascular Cells
Analysis by Dr. Joseph Mercola Fact Checked
Story at-a-glance –
- Researchers used a pseudo virus made of a cell surrounded by spike proteins but without a viral component to demonstrate the spike proteins can damage human cells and alter mitochondrial function
- Many of the long-haul symptoms attributed to COVID-19 may be the result of endothelial damage that triggers poor flow through the capillaries, inflammation and tissue hypoxia
- Data show up to 10% of all people who contracted COVID experienced long-haul symptoms, but none of Dr. Vladimir Zelenko’s patients who were treated within the first five days of infection developed persistent symptoms
- As researchers are seeking another target for future vaccine development, French authorities announced five people developed myocarditis after receiving the Pfizer vaccine. Twelve VAERS reports in the U.S. listed myocarditis
During 2020, many people learned more about coronaviruses, and specifically the SARS-CoV-2 virus that causes COVID-19. Pictures of the spiked virus have been plastered across the news media.
The image is reminiscent of a chain mace, or flail. This was a medieval weapon with a spiked steel ball at the end of a chain or leather strap. The image may be frightening. It turns out researchers believe the spikes are responsible for significant vascular damage leading to severe disease.1
Most people will be infected at least one time in their lives by some type of coronavirus. If the COVID-19 pandemic is the first time you’ve heard about coronaviruses, you should know the first one was discovered in chickens in 1930.2 A few decades later the first human coronavirus was identified.3
Currently, scientists have identified four types of coronaviruses that are endemic and can cause up to 15% of common colds.4 Interestingly, if all coronaviruses have originated in the wild, the rate at which the virus is mutating has accelerated dramatically in 20 years.
In the last two decades, three new coronaviruses have emerged: SARS in November 2002;5 MERS in September 2012;6 and SARS-CoV-2 in December 2019.7 The symptoms of COVID-19 from an infection with SARS-CoV-2 can vary to a great extent.
Some people carrying the virus have had no symptoms. Others report fever, headache, body aches, dry cough, loss of appetite and loss of smell.8 In others, more severe symptoms can develop that affect the respiratory tract and lead to pneumonia.
Approximately 36% of individuals have experienced gastrointestinal symptoms or neurological symptoms, either with or without respiratory symptoms.9 A recent paper published in Circulation Research10 revealed it is the spiked proteins on the virus that play a key role in your symptoms.
Spiked SARS-CoV-2 Damages More Than Your Lungs
A team of researchers including scientists from the University of California San Diego evaluated the effects of the SARS-CoV-2 virus in animals. The researchers were not surprised by the clinical findings, but the data revealed a detailed explanation of how the spike (S) protein triggers damage to the vascular system.11
The researchers created a pseudo virus, or cell surrounded by the spike proteins that did not contain a virus.12 Using an animal model, the researchers administered the pseudo virus into the lungs and found the virus was not necessary to create damage. Instead, the spike protein was enough to cause inflammation.
The experiment was then replicated in the lab using cell cultures. The team exposed healthy endothelial cells that line your arteries to the spiked pseudo virus. Past studies had demonstrated that exposure to the SARS-CoV-2 virus elicited damage to the cells by binding to angiotensin converting enzyme 2 (ACE2).
However, the team found the cells responded in a similar way when exposed to the pseudo virus. When the S protein attached to the ACE2 receptor it disrupted signaling to the mitochondria and caused damage and fragmentation. The alterations in mitochondrial function were confirmed as part of the inhibition of ACE2 signaling in the lab.
The results also revealed that the virus could induce endothelial cell inflammation and endotheliitis. The protein reportedly decreased ACE2 levels and impaired nitric oxide bioavailability.13 Co-senior author of the study, Uri Manor, explained in a press release from Salk Institute:14
“If you remove the replicating capabilities of the virus, it still has a major damaging effect on the vascular cells, simply by virtue of its ability to bind to this ACE2 receptor, the S protein receptor, now famous thanks to COVID. Further studies with mutant spike proteins will also provide new insight towards the infectivity and severity of mutant SARS-CoV-2 viruses.”
Long Haul Symptoms May Be Related to Vascular Damage
Some of the symptoms from COVID-19 that last weeks or months for some people may be the result of vascular damage. People who have had these symptoms have been given the name “long haulers.”15
In theory, they have recovered from the worst symptoms of the illness and test negative. Yet, they continue to have symptoms without an active infection. According to a paper in JAMA,16 approximately 10% of people who have had COVID-19 may experience long haul symptoms.
The Centers for Disease Control and Prevention17 report that a combination of the following symptoms without an active COVID infection can appear weeks after the infection and last for months. Symptoms may worsen after physical or mental activity.
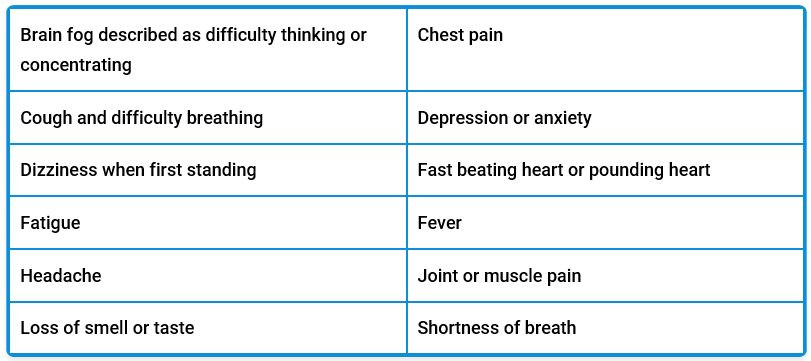
The predominant pathophysiology of COVID-19 includes endothelial damage and microvascular injury, stimulation of hyper inflammation and hypercoagulability.18 A recent review in Physiological Reports19 examined how the capillary damage and inflammation from endotheliitis triggered by COVID-19 could contribute to the persistent symptoms by interfering with tissue oxygenation.
The combined effects of capillary damage in multiple key organs may accelerate hypoxia related inflammation and lead to long haul symptoms. Although exercise temporarily worsens long haul symptoms and some have rejected high-intensity interval training (HIIT) as an option, one paper published in Frontiers in Cardiovascular Medicine from Denmark suggests the opposite.20
The authors of this study argue that the pathophysiology of COVID-19 may be overcome by the physiological effects of HIIT and it should be considered as one of the rehabilitation choices to potentially reverse these symptoms. They propose that exercise could increase viral clearance and modulate TNF-alpha and interleukin-1 beta signaling.
This may in turn reduce vascular inflammation. They acknowledge that HIIT is the most controversial type of exercise intervention to be prescribed after COVID-19, due to the risk of sudden cardiac arrest secondary to cardiovascular damage.
Several experts21,22 recommend even those accustomed to high intensity exercise should first complete a cardiovascular exam and approach their return to physical activity gradually. They cite a small retrospective study of 28 people with a history of COVID-19 in which the researchers concluded that “comprehensive cardiopulmonary rehabilitation after COVID-19 is safe, feasible, and effective.”23
Early Treatment May Reduce the Number of Long Haulers
In my interview with Dr. Vladimir Zelenko in March 2021, we discussed the treatment of COVID-19 with hydroxychloroquine. At that point, Zelenko had treated 3,000 patients with symptoms of COVID-19 and only three of his high-risk patients had subsequently succumbed to the disease.
While the focus of the interview was on treatment protocols and the use of the antimalarial drug hydroxychloroquine, Zelenko shared an interesting statistic about his protocol. In the early months of COVID-19, Zelenko decided to treat his high-risk patients as early as possible, without waiting for severe symptoms. This turned out to be one key to his significant success.
Without waiting for test results that often took five days, by which time high-risk patients were exhibiting more severe symptoms, he started treatment immediately. His understanding of the mechanism behind hydroxychloroquine and zinc led to using the combination alongside azithromycin, to prevent bacterial pneumonia and other bacterial infections common with COVID.
What is interesting are the statistics for Zelenko’s patients with long haul symptoms. As I’ve discussed, approximately 10% of the population that is infected with COVID-19 will go on to experience persistent symptoms.24 However, Zelenko has treated 3,000 patients and none who received treatment within the first five days went on to develop long-haul symptoms.
While he has had patients with persistent symptoms from COVID-19, they sought medical care after the first five days of symptoms, which meant the inflammatory process had advanced. From his experience, and the experience of the patients he treated, early intervention with the protocol nearly eliminated the risk of persistent symptoms.
Researchers Find Another Vaccine Target
During vaccine development, researchers and pharmaceutical companies have focused on the spike protein that surrounds the virus. It appears that this is how the virus enters the cells and it seemed reasonable if the virus could not replicate inside the cells, the infection could be stopped.
However, as has been discovered, the virus has more than just a single spike protein.25 There are four proteins that form the structure surrounding the RNA. There is an envelope (E), a membrane (M) and a nucleocapsid (N), in addition to the spike (S). Your immune system recognizes all four of these proteins. Researchers have discovered humans make more antibodies to the N protein than the S protein.26
However, it seemed counterintuitive to address the N protein since this is found inside the structure with the viral RNA. Therefore, any antibodies your body makes against the N protein will not block the virus from entering the cells.27 New information has revealed that once the N protein antibodies get inside the cell they are recognized by an antibiotic receptor, TRIM21.
This antibody receptor shreds the N protein, which then reaches the surface of an infected cell. Your body’s T cells recognize the fragments and kill the cell along with any virus. This has suggested to researchers that inducing N protein antibodies may be another way of stimulating the immune response against SARS-CoV-2.
Another benefit of focusing on the N protein is that it has a lower mutation rate.28 In other words, as the virus mutates in the wild the current vaccine may no longer have any effectiveness against it, in much the same way that the flu vaccine must be altered each year to address influenza variants. The sequence in the N protein is more stable, so researchers postulate that a vaccine may be effective for a longer period.
List of Current Vaccine Side Effects Is Growing
Early in May 2021, reports from France indicated five cases of myocarditis were found in those who had taken the Pfizer BioNTech vaccine. Myocarditis is an inflammation of the heart muscle that can have lifelong effects as it weakens the muscle and creates scar tissue.29
The national medicines safety agency (ANSM) released their weekly vaccine update, saying “five cases have been declared in France.”30 The agency didn’t feel there was enough information to conclude the vaccine had played a role but would continue to monitor reports.
Over 13.5 million doses of COVID vaccines have been administered in France since April 22, 2021. The ANSM reports 16,030 adverse events from those who had been vaccinated. Israel has also reported several cases of myocarditis after people receive their second dose.
A review of the U.S. Vaccine Adverse Event Reporting System (VAERS) shows 12 reports of myocarditis were recorded in the U.S. by April 30, 2021. According to Our World in Data,31 by April 30, 2021, 30.32% of the population in the U.S. had been fully vaccinated. VAERS also showed there were 157,277 adverse events reported by April 30, 2021.32
These numbers are likely far lower than the actual number of people who have experienced adverse events from the vaccines. Research data33 show health care providers identify and report vaccine adverse events in woefully low numbers. In fact, the Johnson & Johnson COVID-19 vaccine was recently paused to teach doctors how to report vaccine injuries.34 The pause has since been lifted in the U.S.
It is crucial to report a vaccine injury or side effect to VAERS, as the data are essential in helping individuals, doctors and researchers make informed decisions. You can make your own report online or using a PDF by going to the Vaccine Adverse Event Reporting System.35 You’ll find more information about adverse events and how vaccines affect your health at the National Vaccine Information Center.36
Sources and References
- 1, 11, 14 Salk, April 30, 2021
- 2 Journal of the American Veterinary Medical Association, 1931;78:413
- 3 The Pediatric Infectious Disease Journal, 2005;24(11)
- 4 The Pediatric Infectious Disease Journal, 2005;24(11) para 2 under figure 1
- 5 Centers for Disease Control and Prevention, SARS Timeline
- 6 Centers for Disease Control and Prevention, Middle East Respiratory Syndrome
- 7 World Health Organization, April 27, 2020
- 8 Centers for Disease Control and Prevention, Symptoms of COVID-19
- 9 Inflammatory Bowel Disease, 2020; doi.org/10.1093/ibd/iza131
- 10, 12, 13 Circulation Research, 2021; 128:1326
- 15, 16, 24 JAMA, 2020;324(14)
- 17 Centers for Disease Control and Prevention, Post COVID Conditions
- 18 Nature Medicine, 2021;27:601 Pathophysiology
- 19 Physiological Reports, 2021; doi.org/10.14814/phy2.14726
- 20 Frontiers in Cardiovascular Medicine, 2021; doi.org/10.3389/fcvm.2021.643626
- 21 European Journal of Preventive Cardiology, 2020;27(12)
- 22 Netherlands Heart Journal, 2020;28:391
- 23 American Journal of Physical Medicine and Rehabilitation, 2020;99(10)
- 25 C&EN, April 1, 2020, Image of the spiked virus
- 26 Technology Networks, September 10, 2020
- 27, 28 Discover, January 4, 2021
- 29 Myocarditis Foundation
- 30 Brussels Times, May 1, 2021
- 31 Our World in Data, Coronavirus Vaccinations
- 32 OpenVAERS, Covid Data
- 33 Vaccine, 2013;31(24)
- 34 Twitter, Good Morning America, April 14, 2021
- 35 VAERS
- 36 National Vaccine Information Center
From articles.mercola.com