
Entrance to the headquarters of the Centers for Disease Control and Prevention in Atlanta, Georgia (Daniel Mayer/CC BY-SA 3.0)
{kind=link}
The Big Lie about Asymptomatic Transmission of SARS-CoV-2
The media lie that 40% to 50% of SARS-CoV-2 transmission is from “asymptomatic” people while the “fact checkers” facilitate the deception.
“As Virus Spreads, C.D.C. Draws Up an Urgent Battle Plan”, reads the headline of a December 4 article in the New York Times by Rony Caryn Rabin and Apoorva Mandavilli.
“With coronavirus infections soaring across the nation,” the lead paragraph says, “federal health officials on Friday urged Americans in the most forceful language yet to take steps to protect themselves—starting with consistent, proper use of masks—and pressed local governments to adopt 10 public health measures deemed necessary to contain the pandemic.”
The reference is to a policy guidance document published by the Centers for Disease Control and Prevention (CDC) in its journal Morbidity and Mortality Weekly Report (MMWR). The document is titled “Summary of Guidance for Public Health Strategies to Address High Levels of Community Transmission of SARS-CoV-2 and Related Deaths, December 2020”.
The Times quotes the former CDC Director Dr. Thomas R. Frieden, who served under President Barack Obama (while Joe Biden was Vice President), saying that the document shows that the CDC is awakening from its “politics-induced coma”. What it means, according to Frieden, is that public health officials at the CDC are “aligning themselves more with science, which also aligns them more with the Biden administration”.
Further into the article, after again emphasizing the CDC’s policy recommendation on mask use, the Times claims that “asymptomatic individuals. . . are responsible for about 50 percent of transmissions.”
The Times was parroting that claim from the CDC paper, which states that there is “approximately 50% of transmission from asymptomatic persons”.
We may stipulate that this statement does align the CDC more with the politics of President-elect Joe Biden. However, the public must be made to understand that the statement is false and aligns the CDC against the science.
Moreover, the CDC knows that the statement is false.
Additionally, the CDC must surely understand that false claims such as this will be uncritically parroted by mainstream media outlets like the New York Times in ways that serve to manufacture consent for the authoritarian lockdown measures that Biden favors, including business closures or restrictions and executive mask-wearing orders.
The false claim causes people to be irrationally fearful of other people since anyone could be among the “silent spreaders” who never develop symptoms of COVID-19 but who nevertheless efficiently transmit the novel coronavirus that causes it, SARS-CoV-2.
In truth, the scientific evidence indicates that asymptomatic transmission is rare. People who become infected with SARS-CoV-2 but never develop COVID-19 appear not to be a major contributing factor in the community spread of the coronavirus.
There are studies that estimate that individuals who are presymptomatic, meaning that they do go on to develop disease symptoms, are responsible for a large proportion of community spread. Contact tracing studies have documented cases of evident presymptomatic transmission, but we do not know the extent to which this explains community spread. The estimates reported matter-of-factly by the media come from modeling studies that have serious methodological flaws and limitations biasing results artifactually toward a higher proportion of presymptomatic spread.
The CDC also knows that when it produces false claims like this one about asymptomatic transmission, it is not going to be “fact checked” by the media’s self-proclaimed “fact checkers”.
Articles like this one from the New York Times that repeat such false claims are not going to get flagged on Facebook or other social media for spreading misinformation, and users who share the misinformation will not be penalized in social media algorithms or have their account suspended.
While there is certainly misinformation being spread on social media and by alternative online media, it is the government and mainstream media, including self-proclaimed “fact checker” sources, who are the greatest purveyors of lies and deceptions.
I challenge the “fact checkers” to prove me wrong by doing objective journalism for a change and either applying their own standards universally, rather than selectively “fact checking” only information that doesn’t align with certain political agendas, or by abandoning this whole “fact check” charade altogether.
Let’s now take a look at the claim, show why it’s a bald-faced lie, show why the CDC knows it’s false, and expose the incontrovertible hypocrisy of the faux “fact check” sources that engage in censorship of factual information while greatly contributing to the problem of a misinformed public.
Contents
- “Asymptomatic” vs. “Presymptomatic” Transmission
- How the Mainstream Media Misreport the Science
- What the Science Actually Says
- The Relevance of the Distinction Between “Asymptomatic” and “Presymptomatic”
- Asymptomatic Transmission Does Appear to Be Rare
- The Hypocrisy of the “Fact Checkers”
- The Problems with Estimates of Presymptomatic Transmission
- Conclusion
“Asymptomatic” vs. “Presymptomatic” Transmission

Dr. Thomas R. Frieden in October 2008. He was the New York City Health Commissioner prior to serving under the Obama administration as CDC Director. (Photo by Geoffrey Cowley, licensed under CC BY-SA 3.0)
{kind=link}
Where it states in its policy guidance document that “approximately 50% of transmission” is “from asymptomatic persons”, the CDC provides a reference: a modeling study published in the journal PNAS on July 6 titled “The implications of silent transmission for the control of COVID-19 outbreaks”.
That study, however, did not conclude that half of transmission is from asymptomatic individuals. Rather, the authors stated that the results of their study “indicate that silent disease transmission during the presymptomatic and asymptomatic stages are responsible for more than 50% of the overall attack rate in COVID-19 outbreaks.”
The proportion of transmission occurring from asymptomatic individuals shown by the model was just 3.4 percent, assuming that 17.9 percent of infections are asymptomatic, or 6.6 percent, assuming that 30.8 percent of people who are infected never develop symptoms.
To understand the important distinction that scientists draw between “asymptomatic” and “presymptomatic” transmission, we can turn back to the CDC. In a document titled “COVID-19 Pandemic Planning Scenarios” document, which was last updated on September 10 (archived version here), the CDC explains:

In other words, in terms of transmission, “presymptomatic” refers to a person who develops COVID-19 but transmits the virus before their symptoms develop, while “asymptomatic” refers to a person transmits the virus but never develops COVID-19.
That’s an important distinction.
(Note that I am using terms correctly here, whereas public health officials and the media are wrongly referring to asymptomatic individuals who receive a positive PCR test result as “COVID-19 cases”. People without symptoms, by definition, do not have the disease. I explain that and detail the institutionalized scientific fraud related to the use of PCR tests in my article “Facebook ‘Fact Check’ Lies about PCR Tests and COVID-19 ‘Cases’”.)
The CDC’s pandemic planning document gives a “Current Best Estimate” of “50%” for the “Percentage of transmission occurring prior to symptom onset”. That is, the 50 percent figure in this instance refers entirely to presymptomatic—not asymptomatic transmission.
The authors of the CDC policy guidance document were certainly not incognizant of this distinction when they wrote that “approximately 50% of transmission” is “from asymptomatic persons”. In fact, they contradict themselves and show why that statement of theirs is false.
 Further into the paper, they write that, while estimates very, “>40% of persons infected with SARS-CoV-2 might be asymptomatic, and transmission from presymptomatic persons (those who are not symptomatic at the time they transmit infection, but who later experience symptoms) and asymptomatic persons (infected persons who never experience symptoms) is estimated to account for >50% of all transmission.” (Emphasis added.)
Further into the paper, they write that, while estimates very, “>40% of persons infected with SARS-CoV-2 might be asymptomatic, and transmission from presymptomatic persons (those who are not symptomatic at the time they transmit infection, but who later experience symptoms) and asymptomatic persons (infected persons who never experience symptoms) is estimated to account for >50% of all transmission.” (Emphasis added.)
Here, they again cite the PNAS study. So, the conclusion is inescapable that when they wrote that half of transmission occurs from people who become infected with SARS-CoV-2 but who never develop COVID-19, they knew that was untrue.
Assuming the New York Times reporters also read and understood the whole paper they were reporting about, they also knew that the statement is false and yet reported it anyway.

We can conclude that at least one of the two authors of the New York Times article claiming that half of transmission occurs from carriers who never develop the disease certainly knew better.
As I detailed in my August 21 article “How the New York Times Lies about SARS-CoV-2 Transmission: Part 4”, Apoorva Mandavilli was the author of a Times article published on June 9 titled “In the W.H.O.’s Coronavirus Stumbles, Some Scientists See a Pattern”, in which she explicitly acknowledged “the difference between people who are ‘pre-symptomatic’ and will go on to develop symptoms, and those who are ‘asymptomatic’ and never feel sick.”
That similarly didn’t stop her from falsely claiming in the very same article that the proportion of “asymptomatic transmission” that occurs “could be as high as 40 percent”, according to one team of researchers, and “35 percent”, according to the CDC’s pandemic planning document that was current at the time.
 Where she claimed that asymptomatic transmission accounted for as much as 40 percent of community spread, Mandavilli linked to a prior article of hers from March 31 titled “Infected but Feeling Fine: The Unwitting Coronavirus Spreaders”, in which she reported that researchers from Hong Kong suggested “that from 20 to 40 percent of transmissions in China occurred before symptoms appeared.” (Emphasis added.)
Where she claimed that asymptomatic transmission accounted for as much as 40 percent of community spread, Mandavilli linked to a prior article of hers from March 31 titled “Infected but Feeling Fine: The Unwitting Coronavirus Spreaders”, in which she reported that researchers from Hong Kong suggested “that from 20 to 40 percent of transmissions in China occurred before symptoms appeared.” (Emphasis added.)
Thus, Mandavilli knew when she reported the “40 percent” figure as an estimated proportion of “asymptomatic” transmission that she was not telling the truth. She knew that it rather represented an estimated proportion of presymptomatic transmission.
Similarly, the CDC’s “35 percent” figure was an estimate of presymptomatic transmission.
Mandavilli’s main purpose in writing was to criticize an official from the World Health Organization (WHO) who had said during a press conference on June 8 that the data suggested that asymptomatic transmission is “very rare”.
The WHO official’s statement was untrue, according to Mandavilli’s narrative. As the Times told it, the statement “downplayed the role of asymptomatic spread in the pandemic.” It showed how the WHO’s information “sometimes lags behind rapidly evolving research”, according to “experts”. And WHO officials subsequently “walked back the claim, saying it was a ‘misunderstanding.’”
Thus, the message that the New York Times delivered to the public was that “asymptomatic transmission” is very common.
But that Times’ narrative itself was entirely false. Mandavilli was misrepresenting both the WHO official’s statement and the science.

WHO’s technical lead on the COVID-19 pandemic, Dr. Maria Van Kerkhove, speaking during a press briefing on June 8, 2020, in which she described asymptomatic transmission as “very rare” (Screenshot from YouTube)
In truth, the WHO official was not downplaying the role of asymptomatic spread but accurately reporting what the scientific data indicated; far from lagging behind the research back in June, it remains true today that this is what the data show; and the WHO did not walk back the statement.
What really happened was that Dr. Maria Van Kerkhove, the WHO’s technical lead on the COVID-19 pandemic, answered a reporter’s question by explaining that WHO researchers were trying to distinguish between people “reported as not having symptoms” and people who “are in their pre-symptomatic phase, which means it’s a few days before they actually develop severe symptoms.”
When WHO officials had sought to determine whether reported cases “were truly asymptomatic”, they discovered that many were not without symptoms but had “really mild disease”. (This is distinguished by scientists with the term “paucisymptomatic”.)
Detailed contact tracing reports, she explained, were “not finding secondary transmission onward” from cases who tested positive for viral RNA yet remained “truly asymptomatic”.
 The data, she said, indicated that transmission from truly asymptomatic individuals is “very rare”.
The data, she said, indicated that transmission from truly asymptomatic individuals is “very rare”.
While the WHO was constantly looking at the data and was still gathering information, she reiterated, “It still appears to be rare that an asymptomatic individual actually transmits onward.”
What happened next was that numerous media outlets misreported Dr. Van Kerkhove’s statement by taking her to mean also that people who haven’t yet developed symptoms appear to rarely transmit.
That sparked a fierce backlash against Dr. Van Kerkhove from many in the scientific community who proceeded to blame the WHO official for the media’s incompetence.
In response to the overnight outpouring of criticism, Dr. Van Kerkhove joined another WHO briefing on June 9, ostensibly to make “some clarifications” about what she had said that had caused so much controversy, and to clear up the “misunderstandings”.
She explained that there were very few studies doing detailed contact tracing to determine the role of asymptomatic individuals in transmitting the virus and that she had been referring to “two or three” published studies as well as unpublished data from member states conducting contact tracing studies that had found such transmission to be “very rare”.
It’s a “misunderstanding”, she said, to interpret that as meaning “that asymptomatic transmission globally is very rare”.
The media interpreted this as contradicting her earlier statement, but that interpretation makes no sense. She was obviously not saying that the findings of these studies do not inform us about how the virus has spread through the global human population. She obviously did not mean that it appears rare in studies but remains common outside of scientific research.
The only logical interpretation of this is that she is distinguishing between the proportion of transmission that is asymptomatic and the sheer numbers of cases in which this occurs on the global scale. Obviously, even if only a very small proportion of transmission occurs from asymptomatic individuals, that could still add up to a large number of instances in which this has occurred around the globe. This does not contradict her original statement.
Continuing, she also explained that some researchers had used models to try to estimate “the proportion of asymptomatic people that may transmit”, and these models had produced “a big range” of estimates. “But some estimates are [that] around 40 percent of transmission may be due to asymptomatic. . . um. . . but those are from models. And so I didn’t include that in my answer yesterday, but I wanted to make sure I covered that here.”
That could reasonably be interpreted as walking back her prior statement were it not for two important points. First, she was clearly indicating that the WHO places greater weight in the findings of studies that carefully document actual transmission events than in the findings of studies that use mathematical models to make inferences from the underlying data based on whatever assumptions are put into them. Thus, even if we take her words at face value, she was not walking back what she’d said earlier. She was reiterating it.
Second, we cannot take her words at face value because it was not true that models had estimated the proportion of asymptomatic transmission at 40 percent.
As already discussed in the context of the New York Times’ misreporting, the “40 percent” estimate did not represent an estimated proportion of asymptomatic but of presymptomatic transmission.
After the March 31 Times article reported that estimate, the same team of researchers from Hong Kong published a very widely cited modeling study. It is used by the CDC, for example, as a basis for its own “best estimate” of the proportion of transmission that is presymptomatic. Titled “Temporal dynamics in viral shedding and transmissibility of COVID-19”, the study was published in Nature Medicine on April 15.
The researchers, based on their modeling, estimated that 44 percent of transmission is from presymptomatic individuals. They did not produce an estimate of the contribution to community spread from asymptomatic transmission.
One interpretation might be that Van Kerkhove misspoke and had meant “presymptomatic” when referring to the “40 percent” figure, but this is difficult to sustain given the context in which she said it, which rather indicates that she was being intentional in her wording.
Dr. Van Kerkhove was evidently under intense pressure to say something that would enable the public messaging from government officials and the media to continue to falsely characterize asymptomatic transmission as being a common occurrence. That would explain why she chose to adopt the media’s misuse of the term by conflating it deliberately with “presymptomatic”.
 Later in the briefing, she proceeded to distinguish between people who are “truly asymptomatic” and those who are “reported as asymptomatic” but who “have mild disease” or “go on to develop symptoms”—but she did not clarify that the “40 percent” figure was an estimate of spread from people who do go on to develop symptoms. Nor did her colleagues correct her.
Later in the briefing, she proceeded to distinguish between people who are “truly asymptomatic” and those who are “reported as asymptomatic” but who “have mild disease” or “go on to develop symptoms”—but she did not clarify that the “40 percent” figure was an estimate of spread from people who do go on to develop symptoms. Nor did her colleagues correct her.
A colleague of Dr. Van Kerkhove’s then directed people to the WHO’s guidance on mask use for more information about transmission. Left unsaid was how that document, updated on June 5, stated that the available evidence from contact tracing “suggests that asymptomatically-infected individuals are much less likely to transmit the virus than those who develop symptoms.”
 Relatedly, another question was why the three WHO officials presenting the livestream were not wearing masks. Van Kerkhove’s colleague answered that it was “because our studio team has set this up [so] we are able to be more than a meter apart, so we don’t need to wear masks” (emphasis added).
Relatedly, another question was why the three WHO officials presenting the livestream were not wearing masks. Van Kerkhove’s colleague answered that it was “because our studio team has set this up [so] we are able to be more than a meter apart, so we don’t need to wear masks” (emphasis added).
The WHO’s guidance document rightly observed that, “At the present time, the widespread use of masks by healthy people in the community setting is not yet supported by high quality or direct scientific evidence and there are potential benefits and harms to consider.”
The WHO officials also took questions from social media followers watching the livestream. The very first question they took was “What’s the difference between asymptomatic and presymptomatic transmission or people?”
Dr. Van Kerkhove answered the question, prefacing her response by saying that it was “a good question” and acknowledging that the terms were “confusing” because they aren’t used consistently by different groups. “So when we say ‘asymptomatic’, we mean somebody who doesn’t have symptoms and does not go on to develop symptoms. Truly, no symptoms. That’s what we mean when we say this, and when we read this in papers, that’s what we expect to see.” (Emphasis added.)
“Presymptomatic”, on the other hand, “means they have not yet developed symptoms.”
She still did not clarify that she had herself just used the term “asymptomatic” inconsistently and in a way that enabled the mainstream media to greatly misinform the public. Still neither of her colleagues corrected her for having made the false statement.
Following the follow-up press conference by the WHO team, the media roundly reported that Dr. Kerkhove had “walked back” her statement that asymptomatic transmission appears to be very rare, including by “clarifying” that “asymptomatic” people are responsible for as much as “40 percent” of transmission.
There was no attempt by the WHO, to my knowledge, to correct the misreporting.
In the New York Times, Mandavilli reported that Van Kerkhove had clarified that, in her original statement, she had meant people who do not go on to develop symptoms. Mandavilli falsely reported this as the WHO official “walking back” her statement rather than accurately reporting that Van Kerkhove was simply reiterating the very same thing she had said in the first place.
Thus, for the purpose of supporting a false characterization of Dr. Van Kerkhove’s statement as being contradicted by the science, Mandavilli, too, willfully misrepresented that statement by deliberately conflating “asymptomatic” with “presymptomatic”.
 Contradictorily, Mandavilli also falsely characterized Van Kerkhove’s statement as being contradicted by the scientific evidence because “study after study had shown transmission of the virus from people before they ever felt symptoms.” (Emphasis added.)
Contradictorily, Mandavilli also falsely characterized Van Kerkhove’s statement as being contradicted by the scientific evidence because “study after study had shown transmission of the virus from people before they ever felt symptoms.” (Emphasis added.)
Mandavilli made no attempt to explain how it could logically be true that studies contradicted Dr. Kerkhove’s statement given that the WHO official was explicitly excluding presymptomatic transmission from her “very rare” remark.
At the same time, Mandavilli also acknowledged that Dr. Van Kerkhove was distinguishing between the two, which required Mandavilli to justify her own deliberate conflation. To that end, she quoted one of the “experts” criticizing Dr. Van Kerkhove for using the term “asymptomatic” to mean people who never develop symptoms rather than to simply mean “without symptoms” at the time of transmission—as though Dr. Van Kerkhove had not explicitly defined her terms, as though scientists do not distinguish between them, and as though there was no practical significance to the distinction.
Mandavilli perfectly understood that infectious disease experts do consider it important to distinguish between these terms well prior to her June 9 report, which contributed to a manufactured controversy about the WHO official’s “very rare” statement. In her March 31 report, as I detailed in my article “How the New York Times Lies about SARS-CoV-2 Transmission: Part 2”, Mandavilli had similarly characterized the distinction drawn by scientists seeking “to understand the true scope of the pandemic” as a “a largely semantic debate” and ultimately “unimportant” in the public discourse.

The purpose of that New York Times article, as indicated by its headline, was similarly to instill fear into people about “The Unwitting Coronavirus Spreaders” who are “Infected but Feeling Fine”.
Among other outright lies contained in that article for the purpose of fearmongering was that a study of passengers and crew aboard the Diamond Princess cruise ship “bears out” the estimate that 20 percent to 40 percent of transmission is from people who remained “symptom-free”, meaning that they “never developed symptoms”.
As already seen, the 40 percent was rather an estimate of the proportion of transmission that occurs from people who do develop symptoms. More importantly, what was actually reported by the Diamond Princess study , which was published in Eurosurveillance on March 12, was a proportion of asymptomatic infections—not asymptomatic transmission.
Its authors found that 17.9 percent of passengers who tested positive for SARS-CoV-2 were asymptomatic. They hypothesized that asymptomatic individuals may have contributed to transmission on the ship but explicitly stated that “there is no clear evidence that COVID-19 asymptomatic persons can transmit SARS-CoV-2”.
 This is the level of deception we are dealing with when it comes to mainstream media reporting about the COVID-19 pandemic. This type of willful deception from major news outlets like the New York Times is routine, and the consequence is that the public is systematically misinformed in ways that serve to instill the necessary fear into people to manufacture consent for authoritarian policy responses.
This is the level of deception we are dealing with when it comes to mainstream media reporting about the COVID-19 pandemic. This type of willful deception from major news outlets like the New York Times is routine, and the consequence is that the public is systematically misinformed in ways that serve to instill the necessary fear into people to manufacture consent for authoritarian policy responses.
It is understandable that Mandavilli would attempt to justify her own deliberate conflation of the terms by characterizing the distinction as an unimportant semantic debate, but the reason why scientists make the distinction is because it has real practical significance.
As the WHO has pointed out, for one, it’s important for developing appropriate strategies to control transmission, such as informing the definition of “contact” for contact tracing efforts. (The WHO recommends considering people “contacts” if they had contact with an infected person from two days before the infected person developed symptoms.)
It also has practical relevance for the general public. To give a clear example, children are less likely to develop COVID-19 if infected, and, as the WHO observed in a guidance document about modes of SARS-CoV-2 transmission published on July 9, “individuals without symptoms are less likely to transmit the virus than those who develop symptoms.” (Note that this statement includes presymptomatic as well as asymptomatic individuals.)
Consequently, younger children are less likely to transmit the virus than adults, which is obviously important knowledge for determining the appropriateness of school closures.
It matters, not only to scientists but also to policymakers and the general public, whether people who become infected but never develop the disease are largely responsible for community transmission or not.
Electron microscope image of SARS-CoV-2 in cell culture (Image by NIAID, Licenced under CC BY 2.0)
As I mentioned, far from lagging behind the science, Dr. Van Kerkhove’s statement that asymptomatic transmission appears to be “very rare” remains consistent with the accumulated evidence to date.
It is supported, for example, by a large study from the city in China where the SARS-CoV-2 outbreak originated. Published in Nature Communications on November 20, the study is titled “Post-lockdown SARS-CoV-2 nucleic acid screening in nearly ten million residents of Wuhan, China”.
Researchers in Wuhan did a city-wide screening between May 14 and June 1 using reverse transcription polymerase chain reaction (RT-PCR) assays to detect viral RNA in residents. Among eligible residents, which was those aged six years or older, 92.9 percent participated, which amounted to 9,899,828 people.
With this intensive screening program, they identified no new COVID-19 cases. Yet there were positive test results for 300 individuals who were asymptomatic. Among these, 63 percent also tested positive for antibodies to SARS-CoV-2, offering additional evidence that they had indeed been infected.
 Nevertheless, contact tracing of 1,174 close contacts of asymptomatic individuals with evidence of infection revealed none who also tested positive.
Nevertheless, contact tracing of 1,174 close contacts of asymptomatic individuals with evidence of infection revealed none who also tested positive.
The researchers also tried to culture virus from asymptomatic individuals who tested positive, but the results indicated that there was “no ‘viable virus’ in positive cases detected in this study”. Consequently, despite testing positive for viral RNA, none of these individuals appeared capable of transmitting the virus to others.
As the authors stated, “there was no evidence of transmission from asymptomatic positive persons to traced close contacts.” The asymptomatic individuals who tested positive “were unlikely to be infectious.”
I mentioned how the WHO’s June 5 guidance on mask use noted that asymptomatic individuals are less likely to transmit the virus than those who develop symptoms. That document was updated again on December 1 (archived here). It now states that studies have estimated that around 20 percent of people who become infected never develop disease symptoms. Asymptomatic transmission “can occur”, but studies continue to suggest that “asymptomatically infected individuals are less likely to transmit the virus than those who develop symptoms.”
 The WHO cites a systematic review of evidence from contact tracing studies published on the preprint server medRxiv on October 6 titled “Defining the role of asymptomatic and pre-symptomatic SARS-CoV-2 transmission – a living systematic review”.
The WHO cites a systematic review of evidence from contact tracing studies published on the preprint server medRxiv on October 6 titled “Defining the role of asymptomatic and pre-symptomatic SARS-CoV-2 transmission – a living systematic review”.
That review expressed the role of each type of transmission in terms of the “secondary attack rate”, which they defined as “the number of new SARS-CoV-2 infection cases among susceptible contacts of primary cases divided by the total number of susceptible contacts.”
The review also uses the term “asymptomatic case”. Keep in mind that this means a person who received a positive PCR test but never developed COVID-19.
Three studies following up on 17, 91, and 455 close contacts of asymptomatic cases, respectively, found no evidence for asymptomatic transmission—an attack rate of “0%”.
A fourth study following up on 305 contacts of 8 asymptomatic cases identified one secondary case, for an attack rate of “0.3%”.
A fifth study following up on 119 contacts of 12 asymptomatic cases likewise identified one secondary case, for an attack rate of “0.8%”. That study also showed that “close contacts that lived with an index case had 12 times the risk of infection as those who did not live with the index case”.
In other words, asymptomatic transmission, when it does occur, appears much more likely to occur in households rather than public settings—which has great relevance for circumstances in which adults are being ordered to stay at home from jobs and children are kept home from schools by government policymakers.
Indeed, this is a confounding factor in studies using data collected during “lockdown” measures to estimate the proportion of transmission occurring presymptomatically. In terms of how the findings of such modeling studies have been generalized, this biases their results to favor overestimation of the proportion of presymptomatic transmission that would otherwise occur in the broader community setting in the absence of such measures.
As I have previously explained, “It is ironic that this estimated proportion of presymptomatic transmission has been so widely cited to justify lockdown measures when such measures have likely biased the data toward this very result, which could be to a great extent a statistical artifact from this and other biases inherent in the data.”
Returning to the systematic review of contact tracing studies, a sixth and seventh study respectively “indicated an asymptomatic secondary attack rate of 1% and 1.9%”. An eighth followed up on 106 contacts of 3 asymptomatic cases and found 3 secondary cases, for an attack rate of “2.8%”. That study also showed that the attack rate was higher in the household setting, which should come as no surprise.
The ninth and largest study followed up on 753 contacts of asymptomatic index cases and identified one secondary case, for a secondary attack rate of “0.13%”.
Together, the nine studies reported secondary attack rates of “zero to 2.8%”, which compared with secondary attack rates for symptomatic cases of “0.7% to 16.2%”, which suggests that people who are infected with SARS-CoV-2 but never develop COVID-19 “are responsible for fewer secondary infections than symptomatic and pre-symptomatic cases.”
 It remained unknown “whether the low secondary attack rates from asymptomatic individuals result from low infectiousness or a shorter duration of infectiousness.” One clue was that “cases with asymptomatic infection have a shorter duration of RNA shedding than symptomatic individuals.” There remained “limited data on the shedding of infectious virus in asymptomatic individuals to quantify their transmission potential”.
It remained unknown “whether the low secondary attack rates from asymptomatic individuals result from low infectiousness or a shorter duration of infectiousness.” One clue was that “cases with asymptomatic infection have a shorter duration of RNA shedding than symptomatic individuals.” There remained “limited data on the shedding of infectious virus in asymptomatic individuals to quantify their transmission potential”.
The systematic review also emphasized the practical significance of their findings: “Low likelihood of transmission from asymptomatic index cases combined with high symptomatic secondary attack rates emphasizes that, especially in the context of limited resources, approaches should be targeted predominantly on identifying and immediately isolating patients with prodromal or mild symptoms and their contacts . . . .” (Emphasis added.)
In other words, just because a person receives a positive PCR test does not mean that they should be considered infectious, and pursuing policies based on the opposite assumption—as public health officials in the US and other countries have been doing—is a waste of precious resources.
Presumably, most taxpayers would disagree with the New York Times that the distinction between asymptomatic and presymptomatic is an unimportant semantic debate if they understood how the government was wasting their dollars, which could otherwise have been put to more efficient use had the money not been forcibly expropriated from them to be redistributed according to the whims of bureaucrats and their technocrat advisers who view mass testing and indiscriminate lockdown measures as appropriate policy responses.

A ridiculously hypocritical Facebook “fact check” rests its argument on the incorrect conflation of asymptomatic and presymptomatic transmission even though the “fact check” article it cites states that to do so is misleading.
So, how do the New York Times and the CDC get away with falsely communicating to the public that half of all transmission is from infected individuals who never develop COVID-19 when their own primary source put that proportion not at 50 percent but 3.4 percent?
The self-proclaimed “fact checkers” are part of the problem. These sources are not providing a public service by identifying misinformation and correcting the record. Rather, they are demonstrably engaging in censorship and propaganda, pushing the same political agenda of manufacturing consent for authoritarian government responses to the pandemic.
This is illustrated by the hypocrisy of a related article by Health Feedback, a member of the Poynter Institute’s “International Fact-Checking Network”, which Facebook has partnered with ostensibly to fight online “misinformation”.
Published on June 8, the Health Feedback article is titled “People who do not show COVID-19 symptoms can and do transmit it to others; physical distancing and face masks effectively reduce the risk of transmission”. The transparent purpose of that “fact check” article is to advocate the lockdown measures that were implemented by policymakers.
In short, it responded to posts that “went viral on Facebook” but misrepresented Dr. Van Kerkhove’s statement that asymptomatic transmission appears to be very rare. The posts falsely claimed that the WHO official meant that people “without symptoms” rarely spread the virus and fallaciously concluded that therefore the “lockdown” measures were unnecessary. (See the referenced Facebook posts here and here.)
Numerous media sources also falsely claimed that, by “asymptomatic”, Dr. Van Kerkhove meant all people who are “without symptoms” at the time of transmission. On that basis, some suggested that her statement meant that lockdown measures were unnecessary. Sources that Health Feedback identifies as having misinformed the public include MRCTV, The Blaze, Breitbart, Louder with Crowder, The Daily Wire, The Western Journal, and CNBC.
As Health Feedback reasons, “It is inaccurate and misleading to use the word ‘asymptomatic’ to refer to all people who are not showing COVID-19 symptoms, because many such individuals are in fact presymptomatic.”
Further into the article, Health Feedback reiterates, “Describing asymptomatic individuals as people who don’t have symptoms, as several media outlets have done, is inaccurate and imprecise.”
Health Feedback also acknowledges in passing that “there is some indication that asymptomatic transmission may be rare”.
On Facebook, the posts in question are flagged as “Partly False”. It’s true that the WHO official said asymptomatic transmission appears to be very rare, and it’s true that the data do indicate this; but it’s “Incorrect” and “Misleading” to interpret “asymptomatic” to mean anyone “without symptoms” because scientists distinguish between “asymptomatic” and “presymptomatic” transmission.
That much of the “fact check” article is accurate and reasonable. The problem is that this same criterion for identifying “False” information is being applied hypocritically in furtherance of a political agenda.
Health Feedback fails to explain to its readers that the reason so many people had mistaken “asymptomatic” to simply mean “without symptoms” is precisely because that’s how mainstream media sources like the New York Times had long been misusing it.
If you share the links on Facebook to any of the aforementioned New York Times articles asserting that anywhere from 40 percent to 50 percent of transmission is “asymptomatic” or the recent CDC paper in which the claim is made that “asymptomatic transmission” accounts for 50 percent of the spread of SARS-CoV-2, you can rest assured that your post is not going to flagged as “Partly False”.
 It is hardly sensible for Health Feedback and the rest of the self-proclaimed “fact checkers” to give the media a pass for consistently and deliberately misusing the term “asymptomatic” in contexts that serve to instill fear into people, but then when people who oppose the lockdown measures take the media at their word that it includes people who later develop symptoms, to criticize those people for their misunderstanding of the term.
It is hardly sensible for Health Feedback and the rest of the self-proclaimed “fact checkers” to give the media a pass for consistently and deliberately misusing the term “asymptomatic” in contexts that serve to instill fear into people, but then when people who oppose the lockdown measures take the media at their word that it includes people who later develop symptoms, to criticize those people for their misunderstanding of the term.
In fact, it is provable that Health Feedback has no problem at all with the media falsely reporting that “asymptomatic” individuals have been shown to be responsible for a huge proportion of transmission. Indeed, Health Feedback demonstrably approves of media sources spreading that misinformation!
This is evident from an update to the “fact check” article on June 17, which praises certain media outlets for having supposedly “corrected” their reporting.
In the case of the Daily Wire, “correcting” the article meant appending it to include the usual false assertion that Dr. Van Kerkhove had “walked back” her statement.
In the case of The Blaze, “correcting” the article meant appending the headline to include the claim, “WHO clarifies, says asymptomatic spread may account for 40% of transmission”, without any effort to verify that claim and hence without informing readers that this refers to an estimate of presymptomatic transmission.
In the case of Louder With Crowder, “correcting” the article likewise meant updating it to say that the WHO “has since clarified, saying that asymptomatic spread may account for up to 40% of COVID-19 transmission.” (They meant “SARS-CoV-2” transmission. “COVID-19” is the name of the disease, not the virus, but the media along with public health officials continuously misuse that term, too.)
In the case of Breitbart, “correcting” the article meant updating it to say that the WHO “walked back” its claim that “asymptomatic” transmission is “very rare” by stating that, “according to estimates based on models, asymptomatic spread could account for up to 40 percent of COVID-19 transmission.” (They also meant “SARS-CoV-2 transmission”.)
In the case of The Western Journal, “correcting” the article meant updating it to note the distinction between “asymptomatic” and “presymptomatic” and then falsely claiming that this was “an important distinction in scientific jargon that Van Kerkhove failed to make clear during her presentation” at the June 8 press conference (in which she had made it clear). “Asymptomatic individuals, under this definition,” Western Journal misinformed, “may be responsible for up to 40 percent of virus transmissions, the WHO said.”
 In each of these cases of misinformative reporting, Health Feedback praises the sources for having “corrected” their articles by providing “a more complete explanation of the term ‘asymptomatic’ as defined by the WHO.”
In each of these cases of misinformative reporting, Health Feedback praises the sources for having “corrected” their articles by providing “a more complete explanation of the term ‘asymptomatic’ as defined by the WHO.”
The Poynter Institute itself has claimed, in an article purporting to “debunk misinformation”, that the WHO “walked it back” after Dr. Van Kerkhove said that asymptomatic transmission appeared to be “very rare”.
That, as we have already seen, is itself misinformation. The WHO did not walk it back. Rather, Dr. Van Kerkhove reiterated what she had said in the first place about contact tracing studies suggesting that asymptomatic transmission is very rare.
Furthermore, the WHO official claimed that modeling studies estimated the proportion of “asymptomatic” transmission at 40 percent, but studies attributing such a high proportion of spread to people without symptoms are estimates of presymptomatic transmission.
Thus, we have a situation in which a WHO official was scolded for telling the truth that asymptomatic transmission appears rare but then was forgiven by lockdown advocates for telling a lie that enabled the media to continue deceiving the public into thinking that people who never develop COVID-19 are responsible for up to half of the community spread of SARS-CoV-2.
In an instructive example, on Facebook very recently, I witnessed an article being flagged for “False Information”. The article was by Dr. Joseph Mercola, founder of the leading natural health website Mercola.com, and was titled “Asymptomatic People Do Not Spread COVID-19”.
In it, Dr. Mercola reported on the finding of the study in Wuhan, China, that “not a single one of those who had been in close contact with an asymptomatic individual tested positive”.
Further into the article, Dr. Mercola acknowledged that asymptomatic transmission is possible, but, as observed by Dr. Maria Van Kerkhove, appears to be “very rare”.
Dr. Mercola also rightly criticized the CDC for having recently issued the false claim that “asymptomatic people account for more than half of all transmissions.”
He also discussed how a lawsuit had been filed against self-described “Fact Checkers” over censorship of content that discusses the institutionalized scientific fraud of how PCR tests are being systematically misused to diagnose COVID-19 “cases”, the numbers of which in turn are cited to justify authoritarian lockdown measures.
That article could be fairly criticized because its headline doesn’t communicate the nuance that asymptomatic transmission has been documented rarely in other studies in addition to the Wuhan study finding zero occurrences. However, it is far more egregious for mainstream media to claim that up to half of transmission is “asymptomatic”, yet Facebook doesn’t flag those false claims. Furthermore, that is not why Facebook flagged it.
Clicking the button to “See Why” that article had been flagged, Facebook rather told me that “People infected with SARS-CoV-2 can transmit the virus to others, even if they do not show symptoms of the disease . . .”
Thus, while Dr. Mercola was using the term “asymptomatic” to mean people who never developed COVID-19, Facebook’s “fact check” wrongly conflated it with people who “do not show symptoms” in order to rate the article as “False”.
With no shortage of irony, the link provided by Facebook to support that judgment was to the very same Health Feedback article stating that to describe “asymptomatic” individuals “as people who don’t have symptoms” is “inaccurate and imprecise”.
The irony is heightened even further by the passing acknowledgment in the “fact check” article that evidence does suggest “that asymptomatic transmission may be rare”—just as Dr. Mercola had accurately communicated in the text of his article.
The criterion adopted by the “fact checkers” is thus clear: if the term “asymptomatic” is wrongly and deliberately conflated with “presymptomatic” in a way that instills the fear into people that “silent spreaders” who never develop the disease are responsible for up to half of community transmission, then it is approvable; but if the term is in turn used the same way by others who, based on that misunderstanding fueled by the mainstream media’s incessant misreporting, produce content that serves to calm people’s fears, then it must be censored.
Furthermore, even if the content uses the term “asymptomatic” correctly to mean only those who never develop symptoms, if it also emphasizes that studies show that asymptomatic transmission occurs very rarely and rightly criticizes the CDC for issuing a false statement to the contrary, it must be censored.
Young women running with face coverings despite being outdoors where the risk of SARS-CoV-2 transmission is negligible. The WHO advises that “people should not wear masks during vigorous intensity physical activity”. (Photo by Mircea Iancu, from Pixabay)
In summary, it appears that the thought-controlling media do not want there to be widespread understanding that what Dr. Van Kerkhove said was and remains true: the scientific evidence indicates that asymptomatic transmission is very rare.
This is further acknowledged at the end of the Health Feedback article where it quotes five scientists providing their feedback about the matter. The very last expert cited rightly pointed out that Dr. Van Kerkhove had clearly distinguished between asymptomatic, paucisymptomatic, and presymptomatic cases in her original statement that asymptomatic transmission appears to be rare. The expert also acknowledged that “This may well be true.” Detailed contact tracing in Taiwan and Europe, for example, had “suggested that true asymptomatics rarely transmit.”
Despite these acknowledgements contained in the article, the “fact check” approved of media supposedly “correcting” their articles to state just the opposite.
But setting all that aside, we are left with a practical conundrum, which is that, if you are out in public in close contact settings, you cannot know whether people around you might have inapparent symptoms or might go on to develop symptoms within the next couple of days.
As a practical matter, therefore, it still sounds alarming that nearly half of transmission occurs before symptom onset, according to models.
This is why it does make sense to avoid large crowds and close contact with others, which the CDC defines as being within six feet of someone for 15 minutes or more, and to wear a face mask to reduce the risk of droplet transmission as a courtesy to others in situations where close contact is unavoidable.
But what doesn’t make sense is the mass testing regimen in which positive PCR results are being fraudulently used to include individuals with no evidence of disease in the COVID-19 “case” counts, which numbers are in turn continuously cited to justify authoritarian policy responses, or the mandated universal of masks in public settings regardless of individual circumstances.
Furthermore, and with that said, we must also remember that model outputs are dependent upon the input assumptions. One key lesson from the pandemic is that findings from models may have little bearing on reality. Estimates from modeling studies, unlike contact tracing studies, do not represent documented presymptomatic transmission events.
Take, for instance, the modeling study in PNAS cited by the CDC to support its purposefully false claim that “approximately 50% of transmission” is “from asymptomatic persons”.
As already noted, that proportion mostly referred to presymptomatic transmission. Furthermore, that estimate depended on the assumption that, “For symptomatic cases, the incubation period included a highly infectious presymptomatic stage prior to the onset of symptoms.”
The incubation period is the time from infection until the development of symptoms.
The reference cited as the basis for that assumption is the Nature Medicine modeling study also mentioned earlier, but that study has numerous methodological flaws and limitations that give reasonable cause for questioning that assumption.
The first thing to note about it is that the study authors, as they point out, “did not have data on viral shedding before symptom onset”.
 They only had “viral load” data from patients who were already in the hospital and after those patients’ symptoms had already developed. This introduced the problem of patient “recall bias” as to when their symptoms actually started. This was an issue with data from other studies estimating the incubation, as well. The authors acknowledged that recall bias would likely tend toward overestimation of the incubation period, which would in turn bias their findings toward an estimated proportion of presymptomatic transmission that is “artifactually inflated.”
They only had “viral load” data from patients who were already in the hospital and after those patients’ symptoms had already developed. This introduced the problem of patient “recall bias” as to when their symptoms actually started. This was an issue with data from other studies estimating the incubation, as well. The authors acknowledged that recall bias would likely tend toward overestimation of the incubation period, which would in turn bias their findings toward an estimated proportion of presymptomatic transmission that is “artifactually inflated.”
In addition to an estimated mean incubation period, their calculations also depended on an estimate from another study of the mean serial interval, which is the time from symptom onset in a person who transmits the virus until symptom onset in the person to whom the virus was transmitted. If the mean serial interval is shorter than the mean incubation period, it “indicates that a significant portion of transmission may have occurred before infected persons have developed symptoms.”
Their data on the serial interval was relevant to “settings with substantial household clustering” while lockdown measures were in place in China. As the corresponding author, Eric Lau, acknowledged to me, the more frequent and intensive contact within households “results in shorter serial intervals”. This in turn results in a greater proportion of estimated presymptomatic transmission and limits the generalizability of their findings to the broader community setting in the absence of “stay-at-home” orders and other lockdown measures.
Their estimates of the mean incubation period and mean serial interval differed by less than one day and also had overlapping confidence intervals, which are the range of values expressing the probability that the true value falls within that range. In fact, the confidence interval for the serial interval fell entirely within that for the incubation period. They also reported “symptom onset” to the nearest day. Consequently, as noted in a systematic review of estimates on asymptomatic and presymptomatic transmission published on the preprint server medRxiv on June 17, it is “not possible to ascertain if the difference between calculated serial interval and incubation period are true differences, or an artefact of rounding error.”
 It’s also important to note with respect to their data on “viral loads” that when the authors of the modeling study use the term “viral shedding”, they don’t mean that patients were shown to be expelling infectious virus into the environment around them. They mean that PCR tests were used to detect SARS-CoV-2 RNA in patients’ nasal cavity or throat, and from the “cycle threshold” (Ct) value of positive results, they inferred a “viral load” that they then equated with “infectiousness”.
It’s also important to note with respect to their data on “viral loads” that when the authors of the modeling study use the term “viral shedding”, they don’t mean that patients were shown to be expelling infectious virus into the environment around them. They mean that PCR tests were used to detect SARS-CoV-2 RNA in patients’ nasal cavity or throat, and from the “cycle threshold” (Ct) value of positive results, they inferred a “viral load” that they then equated with “infectiousness”.
The PNAS model likewise equated the Ct values from these PCR tests with “infectiousness”.
To understand the problem with this, we can turn to a CDC Frequently Asked Questions page (archived here) that asks, “Can a Ct value predict how infectious an individual with COVID-19 is?”
The CDC answers that question with a blunt “No. Ct values should not be used to determine a patient’s viral load, how infectious a person may be, or when a person can be released from isolation or quarantine.”
So, how can it be that the CDC on one hand states that Ct values should not be used to determine a patient’s viral load while at the same time relying on study that did precisely that to support its own false statement that half of transmission is from people who never even develop COVID-19?
This is institutionalized cognitive dissonance.
PCR tests work by cyclically amplifying viral RNA, if any is present in the sample, until there is sufficient genetic material present to reach the threshold for a “positive” result. The problem is that a positive result just means that viral RNA was detected. It does not mean that the genetic material represents viable virus capable of infection.
Cycle threshold values do, to some extent, correlate with infectiousness, but it is a fallacy to equate the two. A higher number of cycles to reach positivity suggests that little viral RNA was present in the sample, whereas a lower number of cycles suggests more viral RNA was present to begin with. If more genetic material was present to begin with, there is a greater likelihood that it represents viable virus. However, alluded by the CDC’s answer to the question, this is not necessarily so.
As noted in a systematic review published in Clinical Infectious Diseases on December 3, PCR tests “cannot distinguish between the shedding of live virus or of viral fragments with no infectious potential, and it cannot measure the quantity of live virus present in a person’s excreta.”
To determine whether a positive test represents viable virus, scientists use cell cultures to look for cytopathic effects and viral replication. The reviewers therefore considered studies that examined the relationship between PCR Ct values and the ability to culture viable virus.
One study found that at a Ct value of around 28, viable virus was detected in little more than half of test-positive patients (52 percent). Another found a median Ct value of 18.7 to be associated with positive culture while a median value of 27.5 was associated with negative culture. Another found no viable virus in any specimens with a Ct value greater than 30. Another found “no growth in specimens with a cycle threshold greater than 24”.
Now, with that in mind, here are the Ct values reported in the Nature Medicine modeling study for patients whose “viral load” was inferred from PCR tests from samples taken after an imprecisely measured symptom onset.
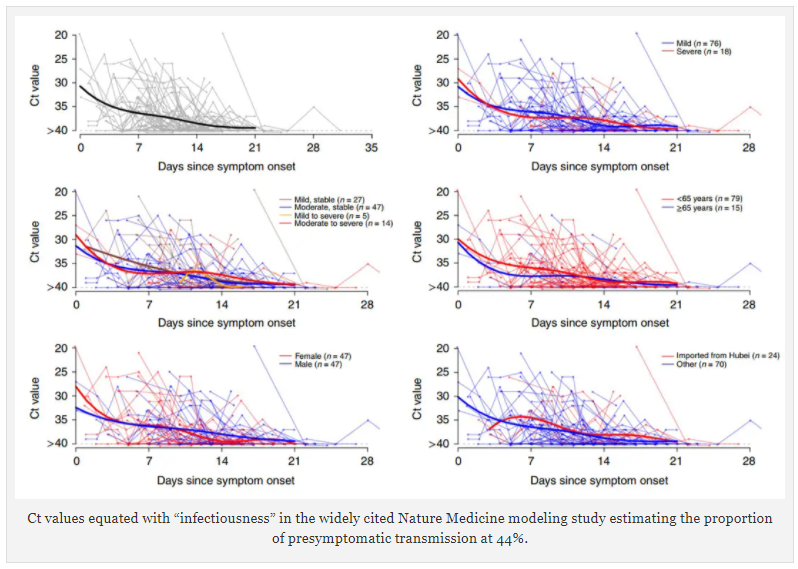
Ct values equated with “infectiousness” in the widely cited Nature Medicine modeling study estimating the proportion of presymptomatic transmission at 44%.
All these graphs show that Ct values generally increased over time since symptom onset, which infers decreasing amounts of viral RNA present in collected samples. Again, they had no data from the presymptomatic phase of infection from any patients. The thick trendlines infer that the “viral load” was generally highest on or around the day that was recorded as being the day of symptom onset, suggesting that patients may have had test positivity at even lower Ct values prior to that day.
The study authors equated Ct values with “infectiousness”, but their graphs also show that, generally, patients with mild to moderate symptoms had test results with Ct values greater than 30, which strongly suggests that most of these patients were not infectious at the time they were tested.
It is theoretically possible that most of these patients had been infectious before they went to the hospital and got tested, but the study did not demonstrate this. Instead, they assumed it.
The major problem with this and other modeling studies, as the preprint review published on the medRxiv observed, is that the data underlying the estimated proportion of presymptomatic transmission is also “compatible with the hypothesis that infectiousness appears to emerge at symptom onset.”
I discussed the numerous other methodological problems with this modeling study in my article “How the New York Times Lies about SARS-CoV-2 Transmission: Part 4”, if you’d like to read more about it. In sum, its flaws bias it in favor of finding a greater period of presymptomatic infectiousness and therefore in favor of an artifactually inflated proportion of presymptomatic transmission.
The CDC nevertheless uses the “44 percent” figure output by the model as a “lower bound” for its estimate of the proportion of presymptomatic transmission in its pandemic planning document.
Tellingly, the CDC, on another Frequently Asked Questions page (archived here), asks, “When is someone infectious?”
The CDC’s answer to that important question is:
It goes on with additional details, but, notably, the CDC says nothing in its answer about current evidence showing that people shed replication-competent SARS-CoV-2 before they develop symptoms.
Conclusion
Let me be clear that I’m not saying that transmission from people without symptoms does not occur. It’s been documented with reasonable certainty in contact tracing studies.
What I am saying is that the evidence, contrary to the deceptive mainstream media narrative being protected by the faux “fact checkers”, does indicate that asymptomatic transmission occurs rarely. So, when you hear claims like “50 percent of transmission is from asymptomatic people”, you can know that you are being lied to.
I am also saying that we still do not really have any good idea about what proportion of community spread is attributable to presymptomatic transmission, and when you hear claims like “40 percent to 50 percent of transmission occurs during the presymptomatic phase of infection”, you should understand that such figures are based on modeling studies that may have little bearing on reality and that rely on underlying data that is consistent with the hypothesis that infectiousness typically begins at the time of symptom onset.
The key takeaway is that the thought-controlling mainstream media are not doing journalism but public policy advocacy, adopting fearmongering narratives that manufacture consent for authoritarian lockdown measures that are of questionable benefit and that indisputably cause massive harm.
The self-proclaimed “fact check” sources, meanwhile, are serving the same purpose by censoring important factual information and criticizing sources that allegedly spread “misinformation” on the basis of criteria that, if applied objectively, would mean that sources like the New York Times and the CDC should get flagged in your Facebook feed for spreading information that is at least “Partly False”.
Such objectivity from the “fact checkers”, I posit, will never happen. I challenge them to prove me wrong by either ceasing their extraordinary hypocrisy or, preferably, abandoning the whole charade altogether.
We do not need these hypocrites telling us what to think and otherwise treating us as though we are too stupid to see through their own untrustworthiness, and we must fight their efforts to prevent members of the public from learning truths that are inconvenient to the authoritarian political agenda they are serving.

About Jeremy R. Hammond
I am an independent journalist, political analyst, publisher and editor of Foreign Policy Journal, book author, and writing coach.
My writings empower readers with the knowledge they need to see through state propaganda intended to manufacture their consent for criminal government policies.
By recognizing when we are being lied to and why, we can fight effectively for liberty, peace, and justice, in order to create a better world for ourselves, our children, and future generations of humanity.
Please join my growing community of readers!

From jeremyrhammond.com